Handbook on Autism
by Cheryl Thacker
This Handbook is the outcome of a masters project completed
by Cheryl Thacker at the University of Saskatchewan.
SSTA Research Centre Report #98-01:117
pages, $17
|
Table of Contents
Introduction
Chapter One - Literature Review
Chapter Two - Teaching Strategies and Techniques
Chapter Three - Case Study
References
Bibliography
Appendix A - Diagnostic Criteria
for Autistic Disorder
Appendix B - Diagnostic Criteria
for Asperger's Disorder
Appendix C - Diagnostic Criteria
for Mental Retardation
Appendix D - Schedules
Appendix E - Social Story for Taking
Turns at the Computer
Appendix F - Special Bibliography
Appendix G - Lesson Plan |
Overview
The Handbook on Autism includes:
-
a review of the literature and major influences in the field
of autism.
-
the aetiology of autism.
-
Aspergers syndrome: considered to be at the higher end of
the autism continuum.
-
hyperlexia: a disorder in where very young children can read
exceptionally well, but often time without corresponding comprehension.
-
practical strategies: Strategies to use in the classroom
and home to increase and improve the social and communication skills of
people with autism.
-
a case study: The life story of a young boy with autism.
The field of autism has a definite, definable history, which
is dealt with in the Handbook. Researchers can not always agree as to what
causes the disorder known as autism, however, it has been proven quite
sufficiently that poor parenting does not cause autism.
This Handbook is intended to be used by parents, professionals,
and people with autism. It is hoped that this Handbook can help, in some
small way, parents, caregivers, and teachers to find some practical answers
to the puzzling condition known as autism. |
Introduction
There is no doubt in anyone's mind, at least those who work with children
and adults challenged by autism, that this particular group of people present
with puzzling, and often times, difficult behaviours. We do not yet know
the specific cause of autism, nor are there any reliable cures for autism.
We do know, however, that by employing various techniques and strategies
with people who have autism, we can reduce excessive behaviours and improve
deficit behaviours (Schriebman, 1994).
Chapter 1 will provide an overview of the disorder known as autism.
It will cover the current thoughts in the field, as well as look at the
history of autism. The aetiology of autism will be explored as well.
Chapter 1 will then focus on the issue of social skill development in
individuals with high-functioning autism. It will address the development
of play skills as well. Some of the current literature regarding social
skill development and play skills will be reviewed.
Chapter 1 will explore Asperger's syndrome. This section will focus
on the history and characteristics of children with Asperger's syndrome.
The phenomena of hyperlexia will also be examined.
The next section of Chapter 1 will focus on the relationship of autism
to mental retardation. Various viewpoints relating to this issue will be
explored. The final section of Chapter 1 will look at the literature regarding
behaviour modification techniques as applied to individuals with autism.
Chapter 2 deals specifically with the strategies and techniques. This
chapter begins by looking at techniques to increase and improve the social
and communication skills of individuals with Asperger's syndrome. Interventions,
such as integrated play groups and social reading strategies will be outlined,
as well as other strategies. Chapter 2 will end with a discussion of behaviour
modification techniques. Many times, the high-functioning individual with
autism engages in inappropriate or self-abusive behaviours. Therefore,
knowledge of basic behaviour modification techniques and principles is
essential for all those involved with individuals who are challenged by
autism.
Chapter 3 presents a case study of a young boy diagnosed with autism.
His past history, diagnosis, and current educational placements will be
outlined. In order for the reader to obtain a general idea of what life
is like for someone who has autism, his personal characteristics and idiosyncrasies
will be detailed,
This handbook in intended to be used by parents, professionals and people
with autism. It is hoped that this handbook can, in some small way help
parents, caregivers, and teachers to find some practical answers to the
puzzling phenomenon called autism.
Many people helped with the completion of this project. A warm and heartfelt
thank you is extended to everyone listed below.
I could not have even begun this project if it were not for my landlords,
who were also my children's caregivers. They looked after me and my children
and gave me the time I needed to study and write this handbook.
My college supervisor was a constant source of encouragement and support.
I learned so much from her. Even long distances did not prevent her from
"being there" for me.
I wish to thank my parents for helping with the children. We appreciated
all the free meals as well!
A special thank you goes out to Betty Fisher. Betty's contribution to
this project was invaluable. Thanks so much, Betty!
Many of the people on the list that follows were kind enough to share
with me their memories of, and stories about the autistic children and
young adults they have worked with over the years. Collecting the "stories"
was perhaps the most enjoyable part of the project for me - listening to
people reliving their happiest and saddest moments with individuals who
have autism reinforced for me that the autistic population is truly incredible
and amazing.
The illustrations found in the handbook were done by Frances Walsh.
Thank you, Frances, for the beautiful pictures.
I cannot possibly list everyone's contribution to this handbook. Therefore,
I will simply list everyone's name and say once more - Thank you very much.
| Jean Bacon |
Barb Bloom |
Wilma Clark |
| Loretta Eldstrom |
Betty Fisher |
Irene Friesen |
| Donald Gallo |
Bruce Gordon |
Velmarie Halyk |
| Connie Hawkemess |
Paulette Lavergne |
Wayne MacDonald |
| Orlene Martens |
Pom Matheos |
Corrie Melville |
| Cassie Olesko |
Bev Poncelet |
Eugene Schumacher |
| Ev Schumacher |
Gloria Stang |
Mary and Ted Thacker |
| Kathryn Whitby |
Gloria Woznik |
Frances Walsh |
And, of course, a big thank-you to "John" and his parents. Thank-you for
letting me enter your lives and for letting me get so close to your family.
I really appreciate all the time you gave to me and I will always remember
my year with "John"!
Back to Table of Contents
Chapter 1
A. is a thirteen year old girl with autism. One Christmas, she was the
Master of Ceremonies at her school's Christmas concert. She was all dressed
up for the occasion with a new pink dress and pair of shoes. The principal
was standing next to her on the stage. He accidentally stepped on her new
shoe, while A. was giving a narration of the Christmas story. A. turned
off the microphone, turned to the principal, looked him in the eye, and
said, "Jesus Christ! Would you get off my new pink shoe!" A. proceeded
to turn the microphone back on, turned towards the audience, and calmly
continued with the narration.
Literature Review
General Overview of Autism
Definitions
Autism is considered a subgroup of Pervasive Developmental
Disorder (P.D.D.). Autism is thought to be at the most severe end of the
P.D.D. continuum (American Psychiatric Association, 1994). Characteristics
of a P.D.D. include an impairment of social interactions, impairment of
communication skills, both verbal and non-verbal and impairment of imaginary
play. Often associated with autism are other symptoms such as: stereotypical
and repetitive repertoires of restricted activities, delayed development
of intellectual skills, impaired comprehension skills, abnormal eating
and sleeping behaviours, inappropriate responses to sensory input, and
self-abusive behaviours. A more detailed list of criteria for diagnosing
autism can be found in Appendix A.
An interesting viewpoint was shared with the world when Clara Claiborne
Park (1982) wrote a book about the first eight years of her autistic daughter's
life. Park defines autism as:
All the autistic child's deficiencies could be seen converging in this
one: the deficiency which renders it unable or unwilling to put together
the primary building blocks of experience. It affects the senses, it affects
speech, it affects action, it affects emotion. The autistic child does
not move naturally from one sound to another, from one word to another,
from one idea to another, from one experience to another. (p. 267)
Back to Table of Contents
CHARACTERISTICS AND HISTORY
Kanner
Autism, by now, has come to be a familiar term in our society.
I believe this is partly due to the movies and other media that depict
such phenomena as
B. is a four year old boy with autism. B. will only eat chocolate
chip cookies. Occasionally, B.'s mom can slip in some extra ingredients,
such as bran, in order to provide a little extra nutrition. However, most
of the time, B. will not tolerate any extra ingredients and will refuse
to eat anything if he detects a new taste in the cookie.
the autistic 'savant' (e.g. the movie RainMan) and best
selling books that describe 'cures' for autism (e.g. Sound of a Miracle:
A Child's Triumph over Autism, Stehli, 1991). I am sure that
most educators could provide a definition or description of autism. However,
most definitions go back to the 'father' of autism, Dr. Leo Kanner. In
1943, Kanner described eleven patients and their behaviours and called
these behaviours "inborn autistic disturbances of affective contact" (p.
250). He was the first to propose that autism could be and should
be a separate diagnosis on its own and not a part of mental retardation
or schizophrenia. Kanner was also the first, it seems, to point out that
autism is present from birth and is, therefore, unlike schizophrenia, which
is an acquired syndrome (p. 242).
Some of the common characteristics that Kanner (1944) lists
as falling under the category of autism include an inability to relate
to people or objects properly, "extreme autistic aloneness" (p. 211), non-existent
or disabled language skills, and the obsessive desire for sameness in the
environment.
Kanner points out that the autistic children he had studied
looked quite normal and he felt they were of average or above-average intelligence
(p. 217). Kanner includes a brief summary of the parents of the children
he had studied and he states that they all appeared to be highly intelligent
although not particularly warm or overly emotional (p. 217). Kanner refrains
from making a
C. is a four year old boy with autism. He very often cries while watching
videos. He gets very sad and puts his head on the floor and weeps. He only
seems to cry when the videos do not have music in them.
a blatant connection at this time, but he does question the
causal relationship between the autistic behaviours and the seemingly cold
parenting styles of the parents of these same children (p. 217).
Rimland
Since Kanner's first descriptions and case studies, people have written
about autism from varying viewpoints. Most writers on the subject will
describe the behaviours and characteristics of autism, all of which resemble
Kanner's first descriptions very closely. Rimland (1964) wrote about autism
more than 30 years ago, and the symptoms he described then remain relevant
today. For example, Rimland's list of autistic characteristics included
such things as trouble with toilet training, abnormal eating patterns,
repetitive behaviours, stereotyped play with objects, insistence on the
same routines, suspicion of deafness and inappropriate speech and language.
Rimland also describes the development of specific skills at an early age,
such as early reading skills or exceptional fine motor skills.
Rimland (1964) writes of the exceptional memory skills of autistic children,
as demonstrated by their replicating their environment in order to maintain
sameness. He also observes that remarkable memory skills are demonstrated
when the individual with autism is able to repeat extraordinary things
often after only hearing it once.
Another characteristic described by Rimland (1964) is above-average
spatial abilities often demonstrated by individuals with autism. This is
most often demonstrated through the swift completion of puzzle tasks.
Rimland (1964) writes about the pronoun reversal commonly heard in the
speech of children with autism. Rimland offers an interesting explanation
for this pronoun reversal. He explains that the:
You-I reversal is clearly an example of what we refer to as closed-loop
phenomena. A sentence such as "Do you want some milk? enters the child's
hearing apparatus, is stored without being disassembled or analyzed, and
later emerges unchanged when an analogous stimulus situation arises. (p.
87)
Park (1982) also has an explanation for the pronoun reversal that is
so common among people with autism. Park feels that by explaining pronoun
usage to the autistic child one only makes the situation more confusing
for the child. Park wonders how any child learns the very complex skill
of pronoun usage in the preschool years. In her mind, normally developing
children and mentally retarded children use their social sense, which the
autistic child does not possess:
The social sense must take over and straighten things out - the sense,
or complex of senses, that assesses the relations of people in a given
situation, how they think of themselves, and consequently what words they
use to identify themselves...What it lacks is that social instinct which
guides even the dullest of normal children in the labyrinth of personal
relations. (p. 206 - 207)
Rimland (1964) describes the prognosis for autism, as it was seen in
1964, as being "closely linked to the speaking ability of the child" (p.
16). This is similar to more current ideas, which indicate that the more
speech an autistic child possesses, the better the prognosis (e.g. Frith,
1989).
D. is an eleven year old boy with autism. The staff at his school
can not leave any type of open containers in his view. D. will urinate
into any open container he sees, even a pop bottle, without making any
kind of mess whatsoever.
Apparently, researchers of autism in the 1960's, were disappointed by
the therapies available to children and parents. Rimland (1964) states
that "autism has not been influenced by any form of therapy" (p. 17). It
seems that families were given opposing advice during the 1950's and 60's.
Kanner was advising that "children raised in warm and affectionate surroundings
tend to do somewhat better...other writers have commented that autistic
children tend to do best in a rigid, minimally stimulating environment"
(Rimland, 1964, p. 17).
Rimland (1964) has studied the characteristics of parents who have children
with autism. Rimland cites case after case that describes either one parent,
or both, as very intelligent and capable. Rimland also found this group
of parents to be obsessive, particular to routines and attentive to details.
However, Rimland views these as positive characteristics, as opposed to
negative influences. He indicates that because these parents were so highly
intelligent, and persistent, they demonstrate much concern and caring for
their autistic children. This was in direct opposition to what Bettleheim
(1967) was saying, around the same time.
Bettelheim
Bettelheim (1967) describes classic symptoms of autism such as "sitting
motionless" (p. 98), mutism or echolalia, self-stimulating movements and
unnatural obsessions with objects (p.98). Bettelheim, unlike Kanner, does
outline definite ideas as to the cause of such autistic behaviours.
He states that "infantile autism is a state of mind that develops in
reaction to feeling oneself in an extreme situation, entirely without hope
(p. 68). He goes on to say "that the precipitating factor in infantile
autism is the parent's wish that his child should not exist" (p. 125).
Bettelheim feels that this rejection by the parents begins with poor breast-feeding
techniques that leaves the baby upset and unfulfilled and the mother feeling
rejected by the baby. This then snowballs into more and more unsatisfying
encounters between mother and child, until finally the baby turns away
from all interactions and begins his/her descent into autism (p. 395).
Bettelheim advocates the removal of these autistic children from their
homes. He himself, placed several children with autism in an institution
and used a combination of 'love' and psychotherapy to bring these children
out of their deeply depressed state. He claims to be very successful at
doing this. He reports that:
Altogether we have worked with forty-six autistic children,
all of whom showed marked improvement. But for purposes of comparison the
following remarks will be restricted to only forty of these forty-six because
one of them (Laurie) was withdrawn after a year; one, unbeknown to us when
we accepted her, had been subjected to a long series of electroshock treatments
a year before she came to us, which precluded effectiveness in our treatment
methods; and four others, at this writing, have not been with us long enough
to make valid assessments
there were eight in our forty for whom the end
results of therapy were "poor" because, despite improvement, they failed
to make the limited social adjustment needed for maintaining themselves
in society
seventeen children whose improvement we classified as "good"
can for all practical purposes be considered "cured"....The fifteen classified
as "fair...are no longer autistic, though eight of them should now be classified
as borderline or schizoid, since they have only made a fair social adjustment.
The remaining seven do much better and only suffer from more or less severe
personality disorders, which limitation has not kept them from making an
adequate social adjustment. (p. 413 - 415)
Rimland (1964) argues against the idea that autism is caused by a cold
and uncaring environment. Rimland strongly advocates for a biological cause
for autism. He sees the parents' unique characteristics as part of the
biological problem and not the cause of the problem.
Park (1982) comments, in her book about her autistic daughter, how it
was that some parents might have appeared cold and unfeeling to professionals.
She talks about meeting with professionals and being extremely disappointed
- Park and her husband were not treated as people, but as a "case". In
one instance with some professionals, Park remembers:
Refrigerator professionals create professional parents, if
the parents are strong enough to keep command of them-selves at all. I
had gone in a highly emotional state, ready to tremble, to weep, to dissolve
in gratitude. Received not even with reproaches, but with no reaction at
all, I of course dried up my emotions at once and met professionalism with
professionalism. (p. 143 - 144)
Nowadays, this idea of parental causation for autistic behaviours is considered
inappropriate and is no longer advocated by professionals in the field
(Kauffman, 1993, p. 212; Tsai & Ghaziuddin, 1992, p.53; Powell, Hecimovic
& Christensen, 1992, p. 191).
Delacato
In the 70's new approaches to dealing with autism appear. Prominent
among them was a sensory-integration type of treatment developed by Delacato
(1974). Delacato's research led him to believe that "These children were
not psychotic. They were brain-injured" (p. 54).
Delacato's (1974) treatment consists of first identifying the "sensoryisms"
(p. 84) of tactility, smell, vision, auditory and taste and then deciding
if the child was hyper or hypo in the sensory experience. The actual treatment
provides either extra stimulation or reduced stimulation to the affected
sensory organs. Delacato claims to have been successful in treating six
out of seven children discussed in his case studies. However, he does state
that "this theory is not presented as a 'cure-all'. Even with this theory
and these practices, I have failures" (p. 167).
Hinerman
More recent writers in the field of autism have been more consistent
when
it comes to describing the characteristics of autism. Hinerman (1983) has
done an excellent review of the various characteristics. She describes
the behavioural characteristics as "slow development or lack of physical,
social, and learning skills
abnormal responses to sensations
abnormal ways
of relating to people, objects and events" (p.5).
E. is a six year old boy with autism. E. is very agile and sure-footed.
E. is able to climb up onto the roof of his house and walk along the edge,
right beside the gutter, without falling off.
Autism is usually defined as involving language impairments as well,
which may include such things as "immature grammatical structure, delayed
or immediate echolalia, pronominal reversal...abnormal speech melody...poor
receptive language...mutism, or a kind of language that does not seem intended
for the purposes of interpersonal communication" (p. 7).
Another major area of dysfunction for the autistic person is the area
of social relationships. They may display a "lack of responsiveness to
people, lack of interest in people, failure to develop attachment to the
mother (as infants), lack of eye contact and facial responsiveness, and
indifference or aversion to affection and physical contact" (p. 8 -9).
Of course, some individuals with autism may display other characteristics
as well, which may include such things as "unusual responses to their environment...an
obsessive attachment to certain objects...aversion to clothing...self-stimulatory
behaviour...stereotyped play patterns...severe disturbances in the development
of perception" (p. 9).
Frith and Baron-Cohen
The prevailing theory in the field of autism today involves
a concept called the 'theory of mind' (Frith, 1989). This theory is very
useful in that it can explain
or give reasons for the apparently bizarre behaviour of many people with
autism. Frith describes theory of mind as a tool that people possess and
use when
F., age thirteen, is diagnosed as a high- functioning person with
autism. One day F. overheard his teacher discussing a book on autism with
another teacher. They were talking about a part of the book which quoted
an autistic child saying she could "hear" her own heartbeat and blood flowing
through her veins. F. turned, looked at his teacher, and asked, "Can't
everyone?"
dealing with others. It is a mental process we go through in our relationships
with other people. It allows us to infer what other people are feeling
and thinking, and lets us predict what may happen next.
Baron-Cohen (1995) defines theory of mind as the ability "to
attribute mental state to oneself and to others and to interpret behavior
in terms of mental states... mental states are unobservable entities that
we use quite successfully to explain and predict behavior" (p. 55)
Frith (1989) proposes that people with autism lack this theory of mind:
The possibility that autistic children lack a theory of mind has been
suggested already on the basis of their peculiar inability to relate to
people in the ordinary way. One implication of this hypothesis is that
autistic individuals are natural behaviorists and do not feel the normal
compulsion to weave together mind behavior for the sake of coherence. (p.
158)
G. is a twelve year old girl with autism. G. can say a few words,
but relies on sign language for the bulk of her communication needs. G.
can finger spell exceptionally well. She watches the learning channel on
TV and has come to school finger spelling such complicated words as "archaeology"
and "Smithsonian".
Baron-Cohen (1995) explains that in order for people to have
a theory of mind mechanism (ToMM), they must also have a shared attention
mechanism (SAM). Baron-Cohen says the shared attention mechanism (SAM)
happens when two people focus their attention on the same object. The SAM
uses "available information about the perceptual state of another person
(or animal)
It then computes shared attentions by comparing another agent's
perceptual state with the self's current perceptual state (p. 45 -46).
Frith (1989) goes on to explain that the "loneliness of the autistic
child does not merely consist of a deficiency in expressing and understanding
emotions. To the autistic individual other mental states, such as knowing
and believing, are equally a mystery" (p. 168).
Frith's (1989) arguments leading to these conclusions are lengthy and
detailed. She compared normally developing children, mentally handicapped
children and autistic children. Her experiments showed that normally developing
children and mentally handicapped children, although different in IQ, could
both identify mental states in others. Because these children had a knowledge
of how the human mind works, they could predict other's behaviours. This
was not the case, however, for autistic children.
Baron-Cohen (1995) and associates have also shown through similar experiments,
that autistic people do not possess a SAM or a ToMM. However, they have
shown that young children and children with intellectual disabilities do
possess both mechanisms. This supports the theory that the basic deficit
of autistic people is their lack of theory of mind.
The theory of mind concept has implications for how we can deal with
individuals with autism. Frith (1989) explains:
H. is a young three year old boy with autism, who cannot talk. H.
has some peculiar eating habits. He will only eat one food at a time, for
days or weeks on end. For example, sometimes H. will only eat potato chips
for one week, then suddenly, for no apparent reason, he will switch to
eating only cookies for a week, and so on.
it would be useful to adopt a literal and behaviorist mode
as a partner of an autistic person, both as listener and as speaker. Implications
need to be spelled out for the autistic person, even if they seem redundant
and self-evident in normal communication....information needs to be actively
solicited since the autistic person may 'forget' to mention an important
fact. (p.180)
Baron-Cohen (1995) discusses ToMM and its relationship to language development.
Baron-Cohen questions which develops first - language or the ability to
read another person's mind? Baron-Cohen argues:
that this drive to inform, to exchange information, to persuade, or
to find out about the other person's thoughts is principally based on mindreading,
and that mindreading is enabled by the language faculty. But by itself,
unless it is hooked up to the mindreading system, the language faculty
may hardly be used - at least, not socially. (p. 131)
Baron-Cohen (1995) feels that we are mindreaders first, then developers
of language. He defines mindreading as the "capacity to imagine or represent
states of mind that we or others might hold" (p. 2). Baron-Cohen supports
his argument that this mindreading ability develops before language by
stating:
consider a person who has an intact language faculty but who cannot mindread
(autism arguably being such a case). Such a person would be able to reply
in perfectly well formed sentences when asked a question like "Where do
you live?" but would be unable to engage in social dialogue - normal conversation.
(p. 131)
Baron-Cohen (1995) stresses that there are many types of autism
and other subgroups many involve more than what he calls "mindblindness"
(p. 1). Mindblindness is being aware of the physical world, but unaware
of mental things; "blind to things like thought, beliefs, knowledge, desires,
and intentions" (p.1). Baron-Cohen suggests that "we need to be careful
about concluding that autism involves mindblindness and nothing else. My
suggestion here is that autism involves mindblindness as a core deficit,
but that other deficits may co-occur" (p. 137).
Aarons and Gittens
Historically, the diagnosis of autism has been problematic. At one time,
researchers and others in the field diagnosed autism on the basis of "all
or nothing" (Aarons & Gittens, 1992, p. 23). Most people in the field
are now moving away from this towards looking at the characteristics on
the
continuum of autism. Aarons and Gittens recommend a "descriptive approach
to diagnosis" (p.23) that includes "observation of children in a social
setting, such as a school or nursery, where their difficulties are more
likely to be highlighted among normal functioning peers" (p. 24).
Another problem with accurate diagnosis of autism is that often the
behavioural troubles exhibited by the child may be attributed to poor parenting.
According to Aarons and Gittens (1992) the problems:
are seen as the outcome of a breakdown in family dynamics,
rather than symptomatic of an underlying disorder. This misinterpretation
of the causes of the child's presenting behavior has brought considerable
distress to many parents who feel that they are being blamed undeservedly
for their child's problems. Yet they are unable to find an alternative
explanation which would make better sense. (p. 25)
What, then, can be done to accurately and consistently diagnose and separate
autism from other handicapping conditions? Aarons and Gittens (1992) offer
a model for diagnosis that includes "looking at the whole child and evaluating
his/her individual difficulties as well as possible abilities and skills"
(p. 30). These authors suggest that professionals in the field look at
several broad areas such as, medical history, early development, appearance,
movement, attention control, sensory function, play skills, basic concept
development, sequencing skills and musical skills.
Back to Table of Contents
AETIOLOGY
Frith (1989) is very firm in her belief that autism, "undoubtedly...has
a biological cause and is the consequence of organic dysfunction" (p. 68).
Sacks (1995) is also a firm believer in a biological cause for autism.
Sacks, a neurologist, has speculated that the aetiology may be genetic
in some cases. Autism may also be associated "in the affected individual
or the family, with other genetic disorders, such as dyslexia, attention
deficit disorder, obsessive-compulsive disorder, or Tourette's syndrome"
(Sacks, 1995, p. 248).
Autism may also be acquired. For example, a number of babies exposed
to the rubella virus during the 1960's later developed autism. They began
to develop normally, then suddenly lost both language and social skills
between the ages of two to four (Sacks, 1995).
Autism could also be caused by a metabolic disorder such as phenylketonuria
(PKU), or a "mechanical" (Sacks, 1995, p. 248) disorder such as hydrocephalus.
Temple Grandin, a person with autism, spoke to Oliver Sacks (1995) about
her thoughts regarding the aetiology of autism. Grandin believes that parts
of her brain are highly developed and are very productive, for example,
the part that controls visualisation. She believes that other parts of
her brain are poorly developed, such as the part that controls verbalisation.
Grandin believes this to be true for most people with autism:
she ascribes this to a defect in her cerebellum, the fact that (as an
MRI has shown) it is below normal size in her. She believes such cerebellar
defects are significant in autism, though scientific opinion is divided
on this. (Sacks, 1995, p. 289)
Grandin questions Frith's (1989) theory of mind as a causal explanation
for autism. Grandin herself:
faces , almost everyday, extreme variations, from over-response to nonresponse,
in her own sensory system, which cannot be explained, she feels, in terms
of "theory of mind." She herself was already asocial at the age of six
months and stiffened in her mother's arms at this time, and such reactions,
common in autism, she also finds inexplicable in terms of theory of mind.
(Sacks, 1995, p. 290 - 291)
Kauffman (1993) notes in his review of the literature, that "autism
is
known to involve a dysfunction of the central nervous system, but the nature
of the dysfunction, remains unknown (p. 181). Tsai and Ghaziuddin (1992)
outline several possible causes of autism, including genetic factors, obstetric
and postnatal factors, neurological factors, and immunological factors.
Although there seems to be no consensus as to one single cause or aetiology
for autism, one thing is clear from the research: "autism is a heterogeneous
behavioral disorder with several different but distinct subtypes" (Tsai
& Ghaziuddin, 1992, p. 67).
J. is a four year old boy with autism. J. can identify his parent's
friends, not by name, but by licence plate number, car make and colour.
J. will approach an adult friend of his parents and simply begin listing
vehicle characteristics - make, model, colour, and plate number, without
prefacing the conversation with a "hello" or "hi". H. is always correct
when matching vehicles to people. J. otherwise does not possess any meaningful
social or communicative speech.
Social Interactions and Impairments
Definitions
Social skills and behaviours can be defined as "the ability
to communicate effectively with people in social and work situations" (Gordon
& Lawton, 1984, p. 179). Social competence can be thought of as "the
progressive capacity for looking after oneself which leads to ultimate
independence as an adult" (Van Osdol, 1972, p. 35).
Lorna Wing defines autism as being a "triad of impairments of social
interaction, communication, and imagination, together with a marked preference
for a rigid, repetitive pattern of activities" (Wing, 1992, p. 129). Wing
further describes the social interaction impairment as having three sub-categories.
One type of social impairment involves children who do not seem interested
in other people at all. They may accept food and drink from people in their
environment, but seem not to view the person as a person, but merely as
a tool for receiving basic need requirements. They are often described
as aloof.
A second type of social impairment that some autistic children may have
is described by Wing as being "socially passive" (Wing, 1992, p. 132).
Children with this type of impairment do not usually initiate social interactions,
but may respond when others do the initiating. They may also copy other
children's movements and behaviours without really understanding the reasons
for the behaviours in the first place.
A third type of social impairment involving children with autism are
those who may initiate interactions with others, but these interactions
are usually bizarre and nonsensical. These children may only talk about
a particular subject or repeat phrases over and over. They may be considered
odd by others.
Characteristics
Children with autism may display any of these characteristics
in different situations. Generally, however, by the age of five or six,
a child with autism will show more tendencies toward one of the subcategories
of social impairments than another.
Children with high-functioning autism also display these characteristics
of social impairments. Usually, such children display characteristics from
the passive or odd subcategories rather than from the aloof category. It
should be noted that children with autism neither lack the ability
to feel emotions nor do they lack the desire to interact with others.
It seems to be more a problem of "an overwhelming difficulty in acquiring
and understanding the multitudinous rules of social life and developing
empathy with others" (Wing, 1992, p. 131).
Children with autism view social interactions differently because of
their trouble understanding social rules and expectations. Some researchers
in this
K. is an eight year old boy with autism. He remembered the order
of presentation of a psychological test given one year previously. He could
remember the order of the subtests he was previously given by a different
psychologist. He told his current psychologist that she was not proceeding
in the correct order when she gave him the same test, but in a slightly
different order.
field feel that children with autism interpret each social interaction
separately. They can not generalise from one situation to another similar
situation. The children are often "left with a series of fragmented social
experiences that are manifested as ritualized, context-specific behaviors"
(Quill, 1995, p. 167). The goal of any treatment program, therefore, is
to make "social interactions more predictable and better understood" (p.
163).
School Problems
High-functioning children with autism encounter problems in
school settings that differ from those who are not high-functioning. Because
of their near-average, average, or superior intelligence levels, they may
not receive many special services in a school setting. These children may
be left on their own to cope the best they can with the complex social
expectations demanded in a school environment. They may have trouble attending
to tasks and may perseverate on their own obsessions during class time.
They may be ridiculed by classmates because of their odd behaviours and
mannerisms. Some high-functioning autistic children, however, have special
interests or obsessions that can lead to relatively successful interactions.
For example, some autistic children excel in music or chess or math games.
These skills can be utilised by school personnel to facilitate appropriate
social interactions (Wing, 1992).
The Normal Development of Play
Why Play is Important
The ability to play promotes social skill growth, among other
things, for young children. Play is fun for most children, but more importantly,
it is how they learn. While engaging in a variety of play situations, children
learn how to solve problems, fine tune their fine and gross motor skills,
learn communication skills and a diversity of social behaviours (Stone
& La Greca, 1986, p. 37).
It is important to know how typical children develop play skills and
how they interact with peers during play periods (Stone & La Greca,
1986, p. 36). This information can be used to compare how children with
autism differ from typical children in this area and "to provide a framework
of normally occurring social skills that could then be utilized in intervention
efforts with autistic children" (p.36).
Vygotsky, a Russian psychologist of the 1920's and 30's, clearly felt
that through play, children develop many skills, including:
the creation of voluntary intentions, and the formation of real-life
plans and volitional motives - all appear in play and make it the highest
level of pre-school development...in this sense can play be considered
a leading activity that determines the child's development. (Cole, et al.,
1978, p.102 -103)
Vygotsky (Cole, et al., 1978) demonstrates that learning does occur
during play by applying his zone of proximal development concept. He states
that in play a child is always operating at a level above his chronological
age. In play, Vygotsky observes, a child acts out skills beyond his everyday,
routine skills. This states Vygotsky, was when learning took place.
L. is a two year old boy with autism. Right now L. is very attached
to a jar of marbles. He takes them everywhere, and has never put a marble
into his mouth. The "object" L. is attached to changes from time to time,
however, he has something beside him at all times. L. even takes his special
"object" to bed with him every night.
Initial Play Development
During a child's first year of life, the purpose of play is
to develop
knowledge about self and significant others in the child's environment.
From birth to around age six months, infants are typically passive interactants
in the play process. They may show appreciation towards the play activities
initiated by parents or others in their environment by smiling and cooing;
however, they do not usually initiate the activities themselves. From age
six months to one year, babies will begin to share interests with familiar
people in their surroundings. They may initiate familiar play routines,
smile and coo to get attention and tentatively begin the sharing process
with toys (Wolfberg, 1995, Stone & La Greca, 1986).
An interesting study done by Lee in 1973 (as cited in Stone
& La Greca, 1986) looked at peer preferences of very young children.
Lee studied infants and toddlers between the ages of eight to ten months
old. He observed them in their typical day-care interactions and he compared:
one infant who was consistently approached by others...to a child who
was avoided. The preferred infant was observed to be more responsive to
social contacts and engaged in more reciprocal interactions with the other
infants. Thus, even at very early ages, the behavioral dimensions of "responsiveness
to others" and "reciprocity" in social interactions appear to be important
indicators of a child's likability. (p. 38)
Pretend Play
Starting around a child's first birthday, pretend play begins
to emerge. Pretend play is the ability to imitate adult behaviours in different
contexts (Wallach & Miller, 1988). Between the ages of one and four,
a child will play "mommy" or "daddy" or imitate the play behaviours of
older siblings and other children. Children at this stage spend time watching
how other children play, imitate the actions of other children and engage
in parallel play with other children (Wolfberg, 1995).
There are several social behaviours that develop in the preschool years
that facilitate positive play interactions between children. Some of these
positive behaviours include such things as "the frequency of smiling and
laughing
sharing and co-operative acts....good eye contact and physical
proximity" (Stone & La Greca, 1986, p. 39).
Co-operative Play
Gradually, co-operative play begins to develop, usually around
the age of four. Co-operative play, that is, sustained play between two
or more children, is a complex process. Children must understand the concept
of taking on different roles; they must adapt their movements and voices
to fit the play situation; and they have to be able to talk about how to
play with each other. As well, children must understand rules regarding
turn-taking. For example, children will typically give each other directions
about what action will happen or when to change play scenarios altogether.
These complex interactions can be thought of as "metaplay" (Wallach &
Miller, 1988, p. 19).
Older Children at Play
Vygoysky (Cole, et., 1978) feels that the nature of
play changes over time. Play starts out as a mere representation of real
life. The young child
M. is a boy with autism who is an escape artist. M. is ten years
old and is non-verbal. On the second day of school, he disappeared from
the school yard during a physical education class. School personnel looked
all over the school grounds and building, but when M. was not found, the
police were called. M. was found downtown, approximately ten kilometres
from the school. He was found by the security guards at a large department
store, in the TV section. No one is sure how M. crossed the streets safely
on his own, as this is not a skill he has successfully demonstrated before.
simply remembers a sequence of events and acts them out. Then play begins
to become more abstract; the child is able to separate the meaning from
the object. Vygotsky felt that play was not as serious for the school-age
child, primarily because school occupies so much of his/her time. However,
others do not agree with this sentiment. According to Wolfberg (1995):
games and sports are the dominant play activities formally
available to children in school and recreation programs while occasions
for make-believe play activities are rare. Nevertheless, the impulse to
pretend in middle childhood continues, particularly when opportunities
for imaginative activities are made available. (p. 200)
Children in elementary school display quite sophisticated play skills.
The sharing and co-operation skills that they learned in early childhood
continue to develop and are important for successful peer relationships.
Children at this age also become more responsive to their play partner's
needs and are more likely to change the play situation to suit their partner's
desires than younger children (Stone & La Greca, 1986, p. 41). School-age
children also learn some new play and social skills such as how to "enter
ongoing peer activities and to extend invitations to peers" (p.41).
According to Vygotsky (Cole, et al., 1978), play changes again, as the
child reaches adolescence. The more mature play of an adolescent helps
to develop abstract thought; ideas and concepts that had not been considered
important before now become dominant.
Many researchers agree that play contains several components that can
be found in various play situations and across age groups (Wolfberg, 1995).
These characteristics include the descriptions that: "Play is pleasurable....Play
involves active engagement in a freely chosen activity....Play is
intrinsically
motivated....Play includes flexibility....Play frequently has
a nonliteral or 'as if' quality" (p. 196).
Autism and the Development of Play
Characteristics
Children with autism have much different play routines and
play
characteristics as compared with the descriptions of typical children's
play
(Stone & La Greca, 1986). All children with autism are different and
each child will display his or her own individual play habits, (or lack
of play habits). There are, however, some common features of the play of
children with autism that can be described. Wolfberg (1995) has researched
the literature and summarises the characteristics in this way:
Overall, they lack the spontaneous and flexible qualities characteristic
of play....When left to their own devices, they commonly impose rigid and
perseverative play routines....Once established, many children with autism
express considerable resistance to a play routine being disrupted....they
tend to exhibit less time and diversity in advanced play skills, fewer
functional play sequences, and fewer symbolic play acts related to dolls
and others....Language, gestures, and sound effects that are indicative
of imagination are rarely spontaneously incorporated
they may repeatedly
construct and reconstruct the same intricate layout of buildings and roadways
but never actually incorporate novel elements into the construction....children
with autism tend to remain on the fringes of peer groups. (p. 201 - 203)
N. is a two year old boy with autism. N. is always full of energy
and loves to climb anything and everything. One day, when his mother had
a visitor in the house, N. climbed to the top of the wall unit, which was
bolted to the wall, and watched the visit from the top shelf.
Children with autism do occasionally attempt to interact with
peers; however, "the limited contact they have is generally negative in
nature" (Stone & La Greca, 1986, p. 46). The reasons for this may be
found in our current understanding of normal social skills development.
Skills such as "mutual visual regard, mutual object manipulation, and imitation"
(Stone & LaGreca, 1986, p.46), which are needed in order to play successfully
with others, begin to develop in very young children. Other skills that
facilitate successful peer
interactions are establishing and maintaining eye contact and playing in
close physical proximity to other children. Children with autism seem to
lack these skills right from the beginning of life.
Symbolic Play
In 1993, Jarrold, Boucher and Smith reviewed the current research
into the symbolic play of autistic children. They found several problems
with the research. The first problem they discussed concerned terminology.
It seems that different researchers use different terms. This makes it
unclear whether each researcher is actually studying the same phenomena
and confuses the issue when conclusions are drawn by comparisons between
studies.
Another problem that Jarrold et al. (1993) found was methodological
in nature. The authors concluded from their review that many researchers
failed to "include control groups or to match control groups adequately"
(p. 295). The authors stated that these shortcomings lead to limitations
in drawing conclusions about "any relative impairment in the symbolic
play of autistic children" (p. 284).
The authors did not dwell only on the negative aspects of the research.
They outlined some firm conclusions that can be found in the research as
well. They stated that the research appeared to point to the fact that
all types of play was impaired in similar ways in autistic children. That
is, autistic children do not typically excel at one type of play over another
type of play. They also concluded from the review that the play of autistic
children seemed to be impaired in all play situations.
Jarrold et al. (1993) concluded their review by discussing the uneven
language abilities characteristic of autistic children and the effect this
may have on studies into play. The authors cautioned that "careful consideration
must be given to the methods used to control for the effects of language
ability" (p. 303).
Normal Language and Communication Development
The Importance of Language
It is often difficult to separate communication skills from
social and play skills. The development and emergence of one affects the
development and emergence of all others. In fact, "communication has been
cited as the foundation of social interaction"
(Stone & La Greca, 1986, p. 47). As in the development of play skills,
it is important to look at the development of communication in typical
children. Then, the language development of autistic children, (or lack
of development) can be looked at in relation to social skill development.
Social Language
The unfolding of a human creature is a truly wondrous event, especially
when one looks at language development. Young infants and toddlers not
only learn and use the semantically, morphologically, and syntactically
correct aspects of language, but they must also:
learn the complex rules of the appropriate social use of language,
what certain scholars have called communicative competence. These rules
include, for example, the greetings that are to be used, the "taboo" words,
the polite forms of address, the various styles that are appropriate to
different situations, and so forth. (Fromkin & Rodman, 1993, p.394)
O. is an eleven year old girl with autism, who seldom talks. Se likes
to work behind a divider at school, so that no one can see her. One day,
while behind a divider, her teacher yawned. The teacher knew no one had
seen her do this, and that O. was hidden from view behind the divider.
However, O. apparently heard the yawn and commented through the divider,
"You tired, teacher?"
One of the first things that a baby learns about language is
how to get the attention of a significant adult in his/her environment.
It has been found that "by the age of 9 to 10 months, infants...initiate
communication through eye contact, physical gestures, and vocalisations"
(Stone & La Greca, 1986, p. 48). From the ages of two to three, the
child's oral language skills increase dramatically. However, the young
child still prefers to use gestures and eye contact as the predominant
means of initiating communication (p. 48).
Preschool Language
As the child enters toddlerhood, many new communication skills
emerge. For example, it has been found that preschoolers will "adapt their
speech in response to listener feedback as well as to specific personal
characteristics (e.g., age, cognitive level, linguistic level) of listeners"
(Stone & La Greca, 1986, p. 50). Preschoolers will also adapt their
responses to feedback from listeners; will ask relevant questions; and
will use language to organise play activities.
School-age Children
School-age children develop and refine their existing communication
skills, as well as develop more sophisticated skills. School-age children
become more effective at using and 'reading' nonverbal communications.
They also are better at both speaking and listening in general; they "become
more adept at eliciting attention and feedback from listeners, and are
able to respond appropriately to explicit verbal feedback (such as questions)
and adapt their speech to the listener's needs" (Stone & La Greca,
1986, p. 52).
School-age children also use their language and communication skills for
reasons that differ from younger children. Children at this stage use language
to initiate play acts, to resolve conflicts, and as an activity in itself;
"social activity becomes important in its own right as a shared peer activity"
(Stone & La Greca, 1986, p. 52).
Autism and the Development of Communication Skills
P. is a nineteen year old young man with autism. When upset, P. will
yell "Call 911 - call 911!", as he did one day in a grocery store when
he temporarily lost sight of his mother. On another occasion, P. was with
his class from school, on a hayride in the country. The driver of the wagon
was driving dangerously fast across the bumpy fields, causing everyone
on the wagon to be bounced around and all were somewhat frightened. P.
kept yelling over and over again, "Call 911 - call 911", until the hayride
ended.
Just as children with autism differ from other children
in many aspects of development, so do they differ in language and communication
skills. Children with autism "are typically late beginning to speak, and
approximately half never develop meaningful speech at all. Those who do
often demonstrate abnormalities in usage as well as delivery" (Stone &
La Greca, 1986, p. 53).
We know that infants and toddlers actively seek attention of others
through the use of eye contact and gestures. However, children with autism
usually fail to develop either of these behaviours, which then leaves them
at risk for not developing higher order skills. For those people with autism
that do develop speech and language, it is often non-communicative in nature.
That is, "conversation is often restricted to the use of stereotyped phrases
and the exchange of concrete pieces of information about limited topics
of interest" (Stone & La Greca, 1986, p. 53).
One can see from the literature regarding language and communication
development, that autistic children's impairment in these areas lead to,
and are undoubtedly connected to, their impairments in other areas such
as social skills and play skills.
Asperger's Syndrome
Hans Asperger was an Austrian psychiatrist, who first described
the condition we now know as Asperger's syndrome (AS) in a 1943 thesis.
Asperger used the term "autism" to describe his patients. This was the
same year that Kanner published his landmark article using the same term.
Asperger's work, however, remained unpublished until 1944, and untranslated
for some time after that. Asperger's work has only become prominent in
the last few years.
Definition
Frith (1991) defines Asperger's syndrome (AS) being made up
of people who:
tend to speak fluently by the time they are five, even if their
language development was slow to begin with, and even if it is noticeably
odd in its use for communication...often become quite interested in other
people and thus belie the stereotype of the aloof and withdrawn child....remain
socially inept in their approaches and interactions. (p. 3 - 4)
Frith (1991) describes people with AS in the following ways: many adults
with AS can function quite well as far as independent living and careers
are concerned. However, they often appear different and awkward. Obsessions
may dominate their lives and topics of conversation. They may appear blunt,
robot-like or cold-hearted. They may engage in stereotypical behaviours
when experiencing stress, similar to lower-functioning people with autism.
People with AS have reported strange sensory reactions, such as hypo- or
hyper- sensitivity to sounds or to the texture of clothes. AS is now included
in the Diagnostic and Statistical Manual of Mental Disorders - 4th
ed (1994). It is called Asperger's Disorder and includes the diagnostic
features of "severe and sustained impairment in social interaction...the
development of restricted, repetitive patterns of behavior, interests and
activities" (p. 75). Also included as characteristics of the disorder are
delayed motor development and clumsiness. The Manual states that the disorder
seems to be more common in boys and than in girls and usually has " a somewhat
later onset than Autistic Disorder, or at least to be recognized somewhat
later" (p. 76). A more detailed description of the diagnostic criteria
used in the Manual can be found in Appendix B.
The term 'high-functioning' is often used in conjunction with AS. There
is confusion in the literature regarding the use of these two terms and
exactly what is meant by each. Szatmari, Bartolucci, & Bremner (1989)
suggest that there is no difference between the two terms. They state that
there are some differences between the two populations "in terms of social
responsiveness, communication and restricted range of activities" (p. 717),
but these differences likely "reflect severity of the disorder rather than
a distinct disorder" (p 717). The authors go on to say that "it may be
best to think of AS as a mild form of HFA [high
functioning autism]" (p.717). For the purposes of this handbook, the
terms Asperger's syndrome (AS) and high functioning autism will used interchangeably.
High-functioning autism, or AS, usually refers to children with autism
who have an IQ score over 70; this "covers close to 20% of the autistic
population" (Levy, 1988, p.2). Frith (1991) considers AS a subcategory
of autism. She sees it as being on the same continuum as autism. Szatmari,
Bremner, & Nagy (1989) hold a similar view, that AS is "on the autistic
spectrum" (p. 559). These authors suggest that AS and autism "share a common
aetiology but differ primarily on severity" (p. 554). Frith (1989) states
that AS should "be reserved for the rare intelligent and highly verbal,
near-normal autistic child" (p. 8).
Characteristics
Some of the characteristics
of the condition, taken from Asperger's own working files, and still considered
in diagnosis today, are such things as:
-
the condition being more common in boys than girls,
-
being not identified in infancy, but usually after age 3,
-
walking may be delayed,
-
speech may occur at normal developmental age, with proper grammar eventually
developing, however, there may likely be evidence of pronoun reversals,
-
language tending not to be used for communication purposes,
-
having limited gestures and limited facial expressions, and limited understanding
of others' gestures and facial expression,
-
possessing abnormal vocal intonation,
-
lacking in understanding of social rules and behaviours,
-
having clumsy and uncoordinated movements, which may affect printing and
drawing skills,
-
may have good rote memory abilities,
-
may develop an obsessive interest in one or two topics,
-
may be teased because of eccentricities,
-
may become aware that they are different than other people and may seek
ways to become more normal-like (Frith, 1991).
Q. is a four year old boy with Asperger's syndrome. One day he was
playing with a small mirror at school. He wanted his teacher to look at
the little telephone in the mirror. The teacher could not understand where
this telephone was, but Q. insisted that it was in the mirror. Finally,
the teacher figured it out. There was a small telephone sticker on the
ceiling above them which the teacher had not noticed before, but obviously,
Q. had. Q. then turned the mirror over to the magnification side and told
his teacher to now look at the big telephone. Q. kept flipping the mirror
from one side to the other and was quite excited about the telephone that
changed size.
Since Asperger's work has come to be known, others in the field
(Wing, 1981; Levy, 1988) have added to the list of distinguishing characteristics
of people with AS. These characteristics include such things as:
-
reduction or complete absence of babbling in infancy and reduction of gestures,
smiles and laughter in early childhood,
-
may not have shown or shared toys with parents and significant others in
environment,
-
lack of ability to engage in pretend play with peers,
-
if play skills do exist, they may lack creativity and flexibility,
-
may relate appropriately with parents and other adults, but not with peers,
-
exhibits a large vocabulary; may know the meanings of difficult and obscure
words, while not comprehending common, everyday words,
-
difficulty with descriptive language and conversational turn-taking,
-
may ask repetitive questions with little concern about the actual answers
to the questions,
-
very concrete and literal, "seldom use colloquialisms, such as 'yea' for
'yes' or idioms, such as 'beating around the bush' " (Levy, 1988, p.4),
-
often display uneven academic skills,
-
lacks common sense,
-
many can be employed successfully in adulthood,
-
may be at risk for psychiatric illnesses in adulthood,
-
may be super-sensitive to criticism by others.
There are certain characteristics of the children that Asperger
described that differ from Kanner's descriptions of children he labelled
as autistic. Asperger described children who developed speech and language
by the time they entered school. They typically had large vocabularies
and demonstrated good grammatical skills. They tended to seek the company
of peers, but did not know how to do so appropriately. Asperger also described
these children as having original thoughts and strange
obsessions (Frith, 1991, p. 96 -97). In contrast, Kanner (1943, 1944) described
children who typically did not speak or, if they did speak, they possessed
a limited vocabulary. And, of course, the children that Kanner described
did not seek the company of peers; in fact they were characterised by "an
extreme autistic aloneness that, whenever possible, disregards, ignores,
shuts out anything that comes to the child from the outside (Kanner, 1943,
p. 242).
Grandin (1995), herself an individual with AS, has described some common
characteristics that people with her condition share. She stated that they
"tend to be good at visual thinking" (p. 47) and may be consumed with anxiety
and nervousness much of the time. Grandin said that the "anxiety felt like
a constant state of stage fright, and caused me to resist changes in routine
because changes made me more anxious" (p. 48).
McLennan, Lord and Schopler (1993) studied a small group of high-functioning
people with autism to see of there were any differences of behaviours between
males and females. Predictably, because of similar studies of other populations,
they found that the males were more handicapped than the females, at the
younger age level. Specifically, the younger females McLennan
R. is a non-verbal, two year old boy with autism. He is an accomplished
escape artist. One night he piled up an assortment of objects, undid the
latch at the top of his bedroom door, and ran away. The police found him
on a busy street in the neighbourhood.
et al. studied were better able to communicate effectively and better
able to initiate social interactions than were the males. This trend was
reversed, however, for older subjects; the males were seen as better communicators
in adolescence and young adulthood. The authors offer a reason for this.
They speculate that the adolescent autistic girl who wants to interact
with her normal peers must typically have good communication and interaction
skills. (Normally developing teenage girls' social experiences consists
of talking and other social interactions.) The autistic girl's weaknesses
are highlighted during these encounters. However, adolescent boys' interactions
tend to revolve around playing sports or watching sports on TV, etc. The
autistic teenage boy does not need as refined communication and social
skills for these interactions.
Prognosis
The prognosis for high-functioning children can be confusing
for parents and caregivers. Some researchers report fairly grim statistics
regarding adult adjustment of high-functioning people. Wing (1981), for
example, reports that of 18 people in her study diagnosed with AS:
4 had an affective illness; 4 had become increasingly odd and withdrawn,...1
had psychosis with delusions and hallucinations...1 had an episode of catatonic
stupor; 1 had bizarre behavior and an unconfirmed diagnosis of schizophrenia;
and 2 had bizarre behavior, but no diagnosable psychiatric illness. Two...had
attempted suicide and 1 had talked of doing so. The rest were referred
because of their problems in coping with the demands of adult life. (p.
118)
On the other hand, Szatmari, Bartolucci, Bremner, Bond, & Rich (1989)
offer a more positive prognosis. They state that the results of their work:
indicate that the grim prognosis often given to parents of young autistic
children may not be universally warranted. A small percentage of nonretarded
autistic children (perhaps those with good non-verbal problem-solving skills)
can be expected to recover to a substantial degree. It may take many years
to occur, and the recovery may not always be complete, but substantial
improvement does occur. (p. 224)
Szatmari, Bartolucci, Bremner, Bond, and Rich (1989) provide some details
of the types of families included in their study. They stress that they
cannot prove the relationship between the family characteristics and the
positive prognosis of their subjects; they simply wanted to report the
anecdotal evidence they gathered. They state that the autistic subjects
involved in the study came from middle-to high-income backgrounds. They
typically had parents, specifically, mothers, who were vocal advocates
for services to meet their children's needs. The authors state that the
"parents worked very hard for their autistic children and often made major
sacrifices in terms of their own family lives" (p. 222).
Problems Encountered by People with Asperger's Syndrome
A common problem for people with AS is the expectations that
others have of them. "The more capable an autistic person appears to be,
the more likely it is that he will be expected to manage his own affairs
without supervision (Frith, 1991, p. 195). However, this is not always
possible. People with AS can get confused and frustrated by these normal,
everyday expectations.
Another problem, as described by Wing (1992) deals with society's perceptions
of high-functioning autistic people. One should not misinterpret the social
awkwardness of high-functioning people with AS to mean that they do not
want to have friends. What seems to be happening is "that their lack of
understanding of the subtle rules of social interaction and communication"
(p. 40) prevents them from forming or even initiating a relationship.
Grandin (1992) makes an interesting observation about the family histories
of high-functioning individuals with autism. From her review of the literature
and from talking to several families in which autism occurs, she has found
that "Family histories of high-functioning autistics often contain giftedness,
anxiety or panic disorder, depression, food allergies, and learning disorders"
(p. 113).
Hyperlexia
Definitions and Characteristics
In the past there has been
confusion as to how to define hyperlexia. In 1976, Elliott and Needleman
reported that there was much confusion in the literature regarding the
definition and diagnosis of hyperlexia. However, one characteristic was
clearly evident in the literature; "The unique characteristic of these
children
is their supernormal sensitivity to visual linguistic symbols.
Production of speech sounds
may be non-existent
or severely retarded, but the unusual attraction to written symbols
is common to all" (p. 346). Elliott and Needleman further report that the
literature, up to that time, was also clear about another characteristic
of hyperlexia; "the interest in written language and ability to read simply
'appeared' upon exposure to written material, much as spoken language appears
after exposure, without the necessity for explicit instruction" (p. 348).
Some definitions of hyperlexia have included all children who
read above their comprehension level. Healy (1982) argues that "many school
children exhibit such discrepancies; to label them all hyperlexic would
be to miss the essential features of this unique condition" (p. 334). Healy
reports in her 1982 study that certain critical features must be present
in order to diagnose hyperlexia. These include:
children who spontaneously read words before age 5 despite disordered
linguistic, cognitive, and interpersonal development. An intense and preoccupying
interest in graphic symbols replaces other developmentally appropriate
activities for these children
.such children may or may not continue to
develop phenomenal word-calling abilities, although word recognition skills
remain well above expectations based on other cognitive or linguistic abilities.
Comprehension on both listening and reading tasks is impaired. While it
may be present for literal units, it breaks down when abstract or organizational
strategies are required to gain meaning. (p. 334)
S. is a two and a half year old boy with autism. S. began to read
at a very young age. He can read brand names on household products and
common logos found in the community. S. can remember and recite commercials
he hears on the television. S. can match the commercials to the proper
products on the store shelf. He does this by singing or repeating the commercial
while pointing to the product or holding the product in his hand.
Aaron (1989) defines hyperlexia a "a reading disorder caused
by severe deficiencies in comprehension accompanied by extraordinary facility
in decoding that has developed spontaneously and at a very young age" (p.
158). Levy (1988) has developed a similar definition, saying that some
high-functioning individuals with autism may have very advanced reading
skills for their age, but their comprehension does not match their reading
level. Other characteristics of the
hyperlexic include: proficient spelling of a limited number of words; precocious
readers of pseudowords; and, may demonstrate understanding of simple sentences,
however, they do extremely poorly on comprehension tasks of complex sentences,
stories and passages (Aaron, 1989).
Other Characteristics
Children with hyperlexia typically begin to develop language normally,
but then may stop speaking at around age 18 months. Other language deficits
include perceiving language differently than normally developing children.
For example, "they perceive language in phrase chunks rather than in words
or morphemes, and they have difficulty comprehending new utterances as
well as generating new utterances of their own" (Kupperman & Bligh,
p. 1). The utterances of hyperlexic children often contain quoted dialogues
and commercials they have witnessed on television or the radio (Kupperman
& Bligh).
These children may also "have an intense need for order,ritual, and
routine. Many also react strongly to touch, smells, and loud noises" (Moses,
1994, p. 25). They may exhibit non-compliance, anxiety, have difficulty
with transitions and with peer interactions (Kupperman & Bligh).
T. is an eight year old boy with autism. T. could read the test instructions
upside down, while being given a psychological assessment.
Prognosis
The prognosis for hyperlexic children is usually positive.
They often have excellent memories and good imaginations which enable them
to do well in school (Moss, 1994).
Working with children diagnosed with Asperger's Syndrome can be rewarding,
as well as frustrating. Because most children with Asperger's Syndrome
often possess the ability to communicate verbally, the opportunities for
interaction are typically greater than with children who function at the
lower end of the autism continuum. Because children with Asperger's syndrome,
however, usually appear like typical children, many people misinterpret
their abilities and expect normal academic and social functioning of them.
In fact, we know that these children do not always do well academically,
and are often very handicapped socially.
Autism: Relationship to Mental Retardation
Definition
The Diagnostic and Statistical Manual of Mental Disorders (4th ed.)
(1994) defines mental retardation quite simply as comprising of three components.
A person must have a significantly sub-average IQ, show significant impairments
of adaptive behaviours, and present with these two characteristics before
the age of 18. See Appendix C for a more detailed list of the criteria
used in
U. is a four year old boy with autism. He knows all the alphabet
letters and can read some words in isolation. He can read all the names
of the children in his preschool classroom. He can read whole books that
he brings from home to share with his teacher and class.
diagnosing mental retardation.
Comorbidity
"Approximately 75% of children with autistic disorder function
at a retarded level...commonly in the moderate range (IQ 35 - 50) (American
Psychiatric Association, 1994, p. 67).
This statistic fits with the information discussed previously regarding
high-functioning autism. Earlier in Chapter 1, it was stated that approximately
20% of the autistic population would be considered high-functioning (Levy,
1988, p.2). With the remaining percentage, anywhere from 70 - 80%, autism
would co-exist with mental retardation. Frith (1991) also agrees with the
above figure, saying that autism can occur at any intelligence level, "although
the majority of those afflicted are mentally retarded, more than half being
in the severely retarded range, even though they may have isolated skills
at a higher level (p. 108).
Myths of the "Hidden Genius"
Frith (1989) discounts the idea that because an autistic person
may excel in one specific area, for example, mathematical computations,
but remains un-testable in other area, that this indicates a generally
high or average IQ level. Frith states that the low IQ scores obtained
by many autistic people reflect their true functioning level. Frith further
explains that in the past the:
IQ was overestimated and misleading if only successfully completed tests
were taken into account. Unfortunately this is often done in practice,
so that the myth of the secretly intelligent autistic child persists. In
particular, children who are found to be untestable on many subtests but
score quite highly on one test tend to be credited with potential they
do not have. It is necessary to take into account of the whole range of
performance in order to make accurate predictions. (p. 83 - 84)
V. is a three and a half year old girl with autism. V. engages in
pica behaviour; that is, she eats or tries to eat non-food items. One day
V. inserted a one-metre cord from a tape-recorder into her throat and stomach.
She pushed it in and pulled it out very smoothly, with no gagging or other
physical response. When V. removed the cord, a large saliva bubble had
formed with which V. then played.
Olley (1992) discusses this idea of the hidden genius of the
autistic child as stemming from Kanner's original descriptions of his autistic
clients. Kanner (1943, 1944) felt that his autistic patients had good intellectual
potential. Olley states that the effects of this notion has been far-ranging:
This myth of the autistic child as latent genius has endured and caused
great distress for family members and teachers who have nearly always failed
to find the key to unlock the alleged genius....research has consistently
found about 80% of people with autism to function in the mentally retarded
range...The remaining 20% show social, language, and other learning problems
that seriously impair their adaptive behaviour. Kanner's optimism about
the intellectual potential of people with autism was sadly unfounded. (p.
4)
Kauffman (1993) and Tsai & Ghaziuddin (1992) would agree with the
above views on the true intellectual ability of persons with autism. Kauffman
states that the "average IQ is probably around 50, with the vast majority
of students falling between about 35 and about 70" (p. 228). Figure 1 shows
the hypothetical distribution of IQ levels in three different populations.
Tsai and Ghaziuddin state that three out of every four autistic persons
also have mental retardation, which supports their idea that autism has
a biological basis, not a psychological basis (p. 53). Furthermore, an
autistic child's IQ level may drop if he or she does not develop useful
language skills by late childhood (Frith, 1989; Kauffman, 1993).
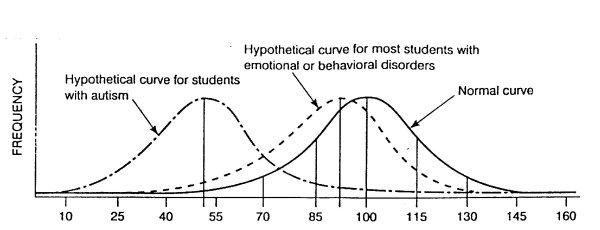
IQ
FIGURE 1
Hypothetical frequency distributions of IQ for most students with emotional
or behavioural disorders and students with autism as compared to a normal
frequency distribution. Taken from Kauffman, 1993, p. 227.
Certain characteristics are thought to be predictive of higher
intellectual levels (DeMeyer, Barton, Alpern, Kimberlin, Allen, Yang, &
Steele, 1974). These authors argue that "children with the capacity to
relate emotionally have the highest adaptive and verbal abilities" (p.
51). These authors also contest the argument that autistic children are
un-testable. They suggest that autistic children are only un-testable when
inappropriate tools are used. DeMeyer et al. go on to say that "most autistic
children are testable when test items within their range of competence
are used; often these must be infant test items" (p. 58).
Divergent Viewpoints
Rimland (1964) argues that autism does not always occur in
association with mental retardation. He gave as a reason for this the fact
that many individuals with autism appear normal-looking. They do not have
the vacant look that many people with mental retardation display, rather,
"they appear always to be concentrating on something else" (p. 10).
Rimland (1964) also found that a characteristic that separates autism
from mental retardation is the exceptional musical ability that is sometimes
seen in
W. is a fifteen year old boy with autism. W. can play a song on the
piano, after only listening to it once on the radio or hearing someone
sing it only once. W cannot read music.
autistic children, which is not often seen in children with mental retardation.
However, Rimland does go on to state that "many autistic children do eventually
become institutionalised as mentally deficient" (p. 13). This, of course,
was a much more common practice when Rimland wrote this, than is practised
today.
Park (1982) had the opportunity to observe mentally retarded
children who were in the same classroom as her daughter, Elly. To Park,
there were vast differences between her autistic daughter and the mentally
retarded children. Park observes that the mentally retarded children were
able to communicate and behave in ways that somewhat resembled normal children.
Her daughter, Elly, who could complete sophisticated math questions, could
not participate in the social world of her peers. Park comments that the
mentally retarded children were "light-years ahead of her in adequacy and
function" (p. 260). So, Park, who did not deny that her autistic daughter
was mentally retarded as well, felt that there was a fundamental difference
between someone who was mentally retarded only, and someone who had autism
as well.
Prognosis
X. is a thirteen year old boy with autism. X. is self-abusive. He bangs
his head with his hand and bangs his head on his wheelchair tray. X. now
has eye cataracts as a result of this abuse.
DeMeyer et al. (1974) found that autistic children with an
IQ score over 50 responded better to educational treatment and remediation.
These authors stress the importance of providing appropriate educational
services "geared to their individual assets and liabilities because some
children in this group have a chance for borderline or even normal functioning"
(p. 59).
Behaviour Modification with Autistic Children
Lovaas' Study
This section of the chapter will look at the literature regarding
the use of behaviour modification techniques with people who have autism.
One technique referred to often in this area was delineated in a study
carried out by Lovaas (1987). His study lasted 15 years. Lovaas claims
he can help autistic children to recover from this disorder. Lovaas states
that "the most promising treatment for autistic persons is behaviour modification
as derived from modern learning theory" (p. 3). Lovaas states that the
positive aspects using behaviour modification techniques with autistic
children includes being able to build complex skills such as language,
and, being able to reduce aggressive behaviours.
Characteristics of the Experimental Children
The children included in Lovaas' (1987) study were all considered
to be classically autistic before treatment. Ten of the children in the
experimental group scored in the severely retarded range on an IQ measure;
seven scored in the moderately retarded and two scored within the normal
range. The children did not possess any pretend play skills; 11 were mute;
seven were echolalic and one possessed limited communication skills. All
the children in the study were younger than four years of age and exhibited
emotional detachment, social isolation and excessive rituals.
Methods of the Study
Lovaas (1987) treated young autistic children, who were under
the age of four, with intensive behaviour modification. Specific techniques
included the use of shaping, positive reinforcement, negative reinforcement,
and various types of punishment. Chapter 2 will outline more fully, specific
behaviour modification techniques, such as the ones Lovaas used in his
program. The study consisted of three groups of children. The experimental
group (n=19) received behavioural treatment for 40 hours per week, for
a two year period. Control group #1 (n=19) received 10 or less hours of
treatment per week, also for a two year period. Control group #2 (n=21)
received no treatment.
Results
Lovaas claimed that nine of the children in the experimental
group recovered, eight were aphasic (difficulty with expressive and/or
receptive language) and two remained autistic or mentally retarded. The
figures for the control groups are as follows:
Control #1 0 recovered; 8 aphasic; and 11 autistic or retarded.
Control #2 1 recovered; 10 aphasic; and 10 autistic or retarded.
Lovaas (1987) considered a child recovered if he or she could
pass grade one in a regular school setting, at the correct chronological
age, and could test within the average or above-average range on an IQ
test.
Training Program
Lovaas' (1981) training program has four basic underlying principles,
all of which reflect Lovaas' philosophy:
-
Deviance from the norm does not necessitate the implementation of unique
treatment methods; "laws of learning apply to individuals with deviant
organic structure as they do to individuals with less deviant structure"
(p. 2 ).
-
The average learning environment works best for average learners; "Persons
at either extreme do not learn well from the average environment because
that environment has not been constructed for them" (p. 2).
-
"Special education and psychology may help those who deviate from the average
by creating and constructing special teaching environments in which the
deviant may learn" (p. 2).
-
This special environment should resemble the child's natural environment
as much as possible; "The smaller the difference between the special therapeutic/educational
environment constructed for the child and the average environment to which,
it is hoped, he will return, the easier the transition" (p.2).
Y. is a four year old boy with autism. At the beginning of the school
year, Y. targeted a student in his preschool class to terrorise. Y. would
attack this other boy for no apparent reason. One day, Y. was sitting at
the table with several of his classmates, including this other boy.
Suddenly, Y. jumped up from his chair, lunged across the table, and began
violently choking the other student.
Lovaas (1987) makes an eloquent statement regarding the cost
effectiveness of intense behaviour modification programs. He states "the
assignment of one full-time special-education teacher for 2 years would
cost an estimated $40,000 in contrast to the nearly $2 million incurred
(in direct costs alone) by each client requiring life-long institutionalization"
(p. 9).
Lovaas (1981) discusses the negative aspects of his program, or, rather,
the mistakes he made when first beginning this project. Through this learning
process, Lovaas incorporated changes into his project which were intended
to improve the teaching and remediation of the autistic children. When
Lovaas and his team first began this study, they treated the children in
a hospital setting.
Lovaas and his team of graduate students found that the children were
not able to generalise the new behaviours they learned in the institution
to their natural environments. Lovaas discovered that the children were
better at generalisation when the treatment was carried out in the child's
own home and preschool environments.
Lovaas (1981) did not include the parents of the children in
the treatment process in the beginning. Lovaas felt that the children needed
the help of professionals and therefore did not enlist the help of the
children's' parents or teachers. Lovaas came to realise that their program
could not be successful unless the parents and teachers were included in
the goal-setting process and the administration of the behaviour modification
techniques.
Lovaas (1981) comments that he expected the children to progress quickly
as a result of the intensive training. He soon realised that these children,
because of their special needs, do not generally make great strides, rather,
"progress followed a slow, step-by-step upward progression, with only a
few and minor spurts ahead" (p. x).
Evaluation of Lovaas' Work
Z. is a fifteen year old girl with autism. Z. is very self-abusive.
Z. pokes her index finger into her eye sockets, so that the whole finger
is inserted into the socket. Z. has damaged her retina doing this. Z. also
bangs her head on hard surfaces, such as brick walls and door frames. Z.'s
head is full of raised bumps from this self-abuse.
The work of Lovaas (1981; 1987) and the publication of his report outlining
his phenomenal successes has raised the criticism of some of his colleagues.
Schopler, Short and Mesibov (1989) have been fairly critical in their review
of Lovaas' work. For example, Schopler et al. point out that Lovaas included
no hard data in his report to back up his claim that a large portion of
the children in the experimental group recovered from autism. Schopler
et al. write that it is not enough to say that a child has recovered from
autism simply because he or she is now placed in a regular classroom. Schopler
et al. claim that more tolerant attitudes towards integration and the fact
that the children in Lovaas' study had full-time advocates could have more
to do with the children's being placed in regular classrooms, than a dramatic
increase in IQ level. Lovaas, Smith, and McEachin (1989), in a rebuttal
to these criticisms, claim that in fact, each child in their experimental
group was dropped from the experiment before entering grade one. They assert
that "These children then entered normal first grade classes on their own
merits. They remained there without any special intervention and were passed
from grade to grade using the same criteria applied to all other children
in such classes" (p. 165).
Schopler et al. (1989) also question the characteristics of the children
chosen for Lovaas' (1987) project. Lovaas claimed that all the children
in his study were classically autistic - some were non-verbal, many were
low-functioning, etc. The gains that Lovaas reports that these low-functioning
children made are surely impressive. Schopler et al (1989) show, however,
through a detailed discussion of the IQ measurements that Lovaas used,
that in reality, the children in the experimental group were likely fairly
high- functioning children with autism. Schopler et al. claim that "The
subjects used in this study were not an average or below average group
of autistic children. Instead, the treatment group was a nonrepresentative,
relatively high functioning group of autistic children with the best prognosis
regardless of treatment" (p. 163).
Lovaas et al. (1989) refute this statement. They claim, through
a detailed discussion of IQ tests and a comparison with previous research,
that the children in their experimental group "did not have a better prognosis
than most children diagnosed as autistic" (p. 166).
Schopler et al. (1989) argue that there are other flaws contained in
the work of Lovaas besides the two mentioned above. They conclude their
review with the statement that "the most conservative conclusion to be
drawn is that it is not possible to determine the effects of this intervention"
(p. 164).
AA. is a twelve year old girl with autism. AA. becomes abusive with
others. She will punch her teacher and teacher associate with her closed
fist when angry. AA. has punched them on the back and on the back of their
legs.
Self-Stimulatory Behaviours
Definition
Lovaas, Newson, and Hickman (1987) discuss the commonly seen
cha
racteristic of self-stimulatory behaviour in autistic children. They
state that the young autistic child experiments with various self-stimulatory
behaviours. Through trial and error, the child eventually perseverates
on only those behaviours that provides him or her with the most perceptual
satisfaction and reinforcement. Lovaas, Newson, and Hickman reviewed the
literature and found support for the notion that self stimulatory behaviour
is self-reinforcing, and thus a learned behaviour. The authors feel that
the strength of the perceptual rewards may interfere with external motivators:
the reinforcing stimuli generated by self-stimulatory behaviour may
be so strong relative to the extrinsic reinforcers controlled by the therapist
or teacher that such extrinsic reinforcers may be relatively ineffectual...
perceptual reinforcers control the individual's attention to such a degree
that he or she attends minimally or not at all to external stimuli. (p.56)
General Strategies
Lovaas, Newson, and Hickman (1987) suggest that teachers, parents
and therapists may gain some control over self-stimulatory behaviours through
the use of an behaviour modification model. They offer three suggestions:
-
employ sensory extinction techniques; in other words, remove the perceptual
rewards in order to produce a decrease in the self-stimulatory behaviour,
-
strengthen alternative behaviours, and,
-
use the self-stimulatory behaviour as a reward for other, more socially
appropriate behaviours. The child can be allowed to engage in self-stimulatory
behaviour upon completion of a designated task. This will only work with
self-stimulatory behaviour that is not harmful to the child or others in
the environment. For example, if a child liked to stroke a certain piece
of cloth, then he or she could be given the special cloth after certain
tasks or behaviours were carried out.
Stimulus Overselectivity
Definition
Lovaas, Koegal, and Schreibman (1979) talk about stimulus
overselectivity, which they say, happens quite frequently in children with
autism. They define stimulus overselectivity as the overselection of:
a limited set of stimuli from those available in their environment....the
children respond to only part of a relevant cue, or even to a minor, often
irrelevant feature of the environment, without learning about the other
relevant portions of that environment. (p. 1237)
Treatment Suggestions
Lovaas, Koegal, and Schreibman (1979) suggest that is this overselectivity
were corrected, perhaps autistic children would learn through more traditional
approaches. They further suggest that discrimination training is
BB. is a thirteen year old boy with autism, who is also hearing impaired.
BB. touches the chalkboard with the tips of his fingers every time he leaves
the classroom, and he touches the stereo in the same manner, every time
he enters the classroom.
the preferred method of eliminating stimulus overselectivity. Lovaas,
Koegal, and Schreibman are vague, however, as to exactly how to go about
this discrimination training. They simply encourage teachers and therapists
to use "sufficient effort and imagination" (p. 1246) in eliminating the
negative effects of stimulus overselectivity.
Conclusion
It seems that in the field of autism there are often more questions
than answers. No single cure has been found. In fact, no two children with
autism display exactly the same characteristics. Several facts are clear,
however, regarding the research literature concerning autism. One is the
fact that many individuals with autism are also intellectually disabled.
Educators must not assume a high level of functioning in individuals with
autism because of possible islands of competence. An autistic child may
seem to be functioning at a normal or above-normal level of intellectual
ability because of good verbal skills or exceptional mathematical ability.
However, this same child likely is functioning at a below-normal level
in most other areas.
Another critical fact that seems clear from the research into autism,
is that
CC. is a four year old boy with autism. CC. engages in very ritualised
behaviours when eating. He lines up the cereal boxes, bowls, cutlery, etc.,
in the same order every day. His mother has to remove her watch so he can
place it in the line-up as well. CC. plays with his toys in the same manner
- lines them up on table edge or wall border. CC. likes to push a doll
stroller repeatedly around the schoolyard at his preschool or in his own
backyard. He will do this for hours at a time and will have a tantrum when
interrupted.
while there is no cure for autism, there is hope for remediation. Many
children and adults with autism can learn to carry out tasks and to function
as independently as possible. Educators must provide the best educational
program possible, one which will enable their students with autism to grow
and to learn and to become optimally functioning adults in our society.
In spite of the above findings, many children with Asperger's
syndrome can lead successful lives as adults. We have many examples of
this today. Temple Grandin (1992, 1995) and Donna Williams (1992) are both
successful high-functioning adults with autism. In order to help people
with autism to function optimally, intervention must begin early; and it
must be appropriate for each specific child's needs. Our educational goal
should be to increase the likelihood of successful adult adjustment for
people with Asperger's syndrome. Teachers and parents of children with
Asperger's syndrome are encouraged to seek out the best educational practices
available to date and to implement individual programs which will enhance
the growth and development of their child with Asperger's syndrome.
DD. is an eight year old girl with autism. DD. is in a classroom
with seventeen other special needs students. For two days, near the beginning
of the school year, the teacher could not figure out what was going on
during the lunch hour. Not one child in the classroom seemed to have a
dessert in their lunchkits. On the second day, the teacher figured it out
- DD. had taken every dessert out of each of the lunchkits in the morning,
and stashed them in her own lunchkit and brought them out at noonhour.
DD. lined them up on her desk and began to eat them, before she was stopped.
It is also clear from the literature that many individuals with autism
exhibit inappropriate and at times, unmanageable behaviour. The research
literature indicates that the predominant treatment for these individuals
is the use of behaviour management techniques. It is important for the
practitioner to have a basic knowledge of behaviour modification techniques.
It is more important, however, for the practitioner to know when and how
to use these techniques. Every individual with autism will present with
different characteristics and different behavioural issues. The practitioner
will need to know how to decide which behaviours should be worked on first,
which techniques would be most effective in altering behaviour, and when
to change or add to the treatment program.
Chapter 2
Teaching Strategies and Techniques
Introduction
One day, a seven year old with autism, was asked by his teacher
assistant to talk in a quiet voice, as his loud voice was disturbing the
class. The boy replied, I hate quiet - I need more voice!"
Perhaps the most debilitating handicap for people
with autism in general, and AS in particular, is their lack of social awareness
and lack of social skills. People with AS need to be taught, explicitly,
the required social rules and etiquette for getting along with peers in
a variety of contexts. They do not learn the appropriate behaviours by
watching others and mimicking correct behaviours. Teachers of children
with AS cannot assume that their students already possess a basic foundation
of social skills in hopes of teaching higher order social skills. Teachers
and others working with these children must assess at what level the skills
are breaking down, and begin instruction, very often, at the primary levels.
This chapter will begin by discussing general teaching
strategies and considerations that practitioners should find useful when
working with children challenged by autism and Asperger's syndrome. Next,
communication and language development will be addressed. Finally, specific
techniques and strategies for the development of social skills will be
outlined.
General Guidelines
Wing (1981) has developed some general guidelines for
the management of people with AS. She suggests that teachers, parents,
and others involved in the autistic person's life should:
-
keep to a regular, predictable routine,
-
keep to the concrete rather than the abstract,
-
try the use of behaviour modification techniques,
-
develop an appropriate educational program in order to develop
existing skills and abilities that may lead to eventual employment, and,
-
treat psychotic illnesses appropriately, if they appear.
Grandin (1992) has observed that "some of the
most successful high-functioning autistics have directed childhood fixations
into careers....Fixations can be tremendous motivators. Teachers need to
use fixations to motivate instead of trying to stamp them out" (p. 115).
She also has developed a list of teaching suggestions for teachers and
parents that apply to high-functioning people with autism. Some of Grandin's
(1995) suggestions include:
-
Use visual methods of teaching and avoid long strings of
verbal information. People with autism often communicate better with the
written word. Introduce typewriters and word processors at an early age....
-
Direct and broaden fixations into useful activities....
-
Develop talent areas such as drawing, music, and computer
programming....
-
Sensory integration therapy from an occupational therapist
should be made available to children with autism....
-
Mainstreaming and meaningful contact with children who have
normal social behavior is essential if a child with autism is to learn
social skills....
-
Early intervention improves the prognosis....
-
A structured, predictable classroom environment helps children
with autism learn....
-
Exercise can help reduce disruptive behavior....
-
Sensible use of behavior management techniques is part of
a good treatment program....
-
The correct medications used properly can improve both behavior
and the quality of life. (p. 49 - 50)
Classroom and Teaching Guidelines
There are many other ways a classroom teacher can help the person
with AS to function more appropriately and effectively within the classroom.
The following are concrete and practical suggestions for the classroom
teacher that may help the student with AS to fit into the classroom community.
Many of the ideas have been adapted from the work of Karen Williams (1995),
of the University of Michigan Medical Center Child and Adolescent Psychiatric
Hospital.
Daily Skills
A seven year old boy with autism often talks in "book language".
After listening to a particular story, he may decide to speak to others
in his environment using the same story pattern he has just heard. For
example, after hearing the story, The Three Little Pigs, the boy
would respond to a request by his teacher or teacher assistant by saying,
"No, no. Not by the hair of my chinny chin chin."
The child with AS is sensitive to changes in his or her
daily environment. The teacher should try to keep transitions to a minimum
and to avoid surprises. When possible, the teacher should prepare the AS
child in advance of any changes to the regular schedule. When the AS student
must change programs, classrooms, schools, etc., he or she should be allowed
to visit the new site, meet the new personnel and become familiar with
the expected routines.
The AS child is usually gullible and naive and often the target of
other students teasing. The classroom teacher may have to protect the AS
student from the bullying and teasing tactics of others. Williams (1995)
suggests teaching the classmates of the AS student about the disability
and enlisting their help in assisting the AS student with learning social
rules, etc. She also suggests pairing the AS student with a peer who can
help the AS student during the day, help focus him or her on tasks, and
involve him/her in social activities.
The classroom teacher will have to watch what the AS student is doing
at all times. AS children like to be left alone to pursue their own interests
and to enjoy their rich inner, fantasy life. However, the classroom teacher
should encourage the AS student to remain involved with classmates as much
as possible during the school day.
Obsessions
The AS student will often want to dominate classroom discussions by perseverating
on his or her particular interest or obsession. One way of dealing with
this is to limit the amount of time the AS student is allowed to talk about
his or her topic of interest. The classroom teacher can specify or timetable
a period of time each day that the AS student will be allowed to talk or
ask questions about his or her interest. The AS student should not then
be allowed to perseverate on his or her topic during other parts of the
school day.
Some children with AS are very stubborn about completing homework, to
the point of refusing to do any work not related to their particular obsessions.
Williams (1995) stresses that:
Firm expectations must be set for completion of classwork. It must be
made very clear to the child with AS that he is not in control and that
he must follow specific rules....however, meet the children halfway by
giving them opportunities to pursue their own interests; For particularly
recalcitrant children, it may be necessary to initially individualize all
assignments around their interest area...Gradually introduce other topics
into assignments. (p. 11)
Attention
Children with AS often experience difficulty with concentration and focused
attention. A strategy to help with this area is to time the student's work
sessions, with the expectation that incomplete work or carelessly completed
work will be made up during recess or some other strategic time period.
Timing AS students helps to organise themselves and also breaks the work
into smaller units which are more manageable for the AS student.
Co-ordination Skills
The AS student is often poorly co-ordinated in both fine and gross motor
skills. Regardless, exercise is an important component of the AS student's
educational program. Grandin (1995) has already mentioned the impact that
exercise can have on reducing excessive behaviour problems. The AS student
will benefit from a fitness-type of physical educational program as opposed
to participating in a competitive sports program. There can be problems
if an AS student is required to participate on a team; "his or her poor
motor coordination may only invite frustration and the teasing of team
members. The child with AS lacks the social understanding of coordinating
one's own actions with those of others on a team" (Williams, 1995, p. 13).
One strategy that will help the AS student with handwriting skills is
to teach him or her the verbal prompts to form the letters (e.g. a = small
circle with a stick). The AS student will likely memorise these verbal
prompts quickly, and can then use them to remind him or her of the correct
letter formations during independent work sessions.
Emotions
One day a seventeen year old girl with autism was at the computer with
her teacher. Suddenly, the girl raised her arm in front of her, and brought
it back towards the teacher. The girl continued to swing her arm into the
teacher. The teacher was knocked backwards off her chair, and somersaulted,
still backwards, across the classroom floor.
The person with AS typically is anxious and stressed by many
factors in his or her environment. The AS student is prone to emotional
outbursts and tantrums because of this. One way to prevent outbursts is
to make the AS student's environment as predictable as possible. Another
tactic is to teach the AS student how to cope with stressful situations.
The AS student can be shown how to take deep breaths in order to relax
the body, to count to ten before responding, etc. The stress-reducing steps
can be written on a card or small piece of paper and given to the student
to carry as a visual reminder.
Finally, it is extremely important that the AS student is paired with
a staff member that is available to check on the student daily. This is
especially critical for the mainstreamed high-school student. The staff
member needs to check how the AS student is coping with various elements
of the high school environment, how the AS student seems to be coping emotionally
and if further assistance or programming changes need to take place. Williams
(1995) stresses that the AS student "must receive academic assistance as
soon as difficulties in a particular area are noted. These children are
quickly overwhelmed and react much more severely to failure than do other
children" (p. 15).
Helping Children Develop Their Communication Skills
One of the most important areas that need remediation in children with
AS is the area of communication. Although children with AS typically possess
language skills, they often do not use language to communicate effectively
or to engage in the social aspects of communication. They have a basic
disorder of pragmatics (Twatchman, 1995). Twatchman (1995) offers many
remedial suggestions for use with high-functioning children with autism.
Some of her ideas will be briefly discussed next:
-
Use the child's strengths and interests to encourage language growth. For
example, if a child is interested in trains, then use trains to facilitate
language growth.
A fifteen girl with autism was with her class on a field trip to
a large shopping mall. The girl was talking constantly, to everyone in
her group,
and even to people not in her group. While she was walking along
the mall corridor, she was talking to the principal and not looking where
she was going. She walked into the water of a fountain. Without stopping
to catch her breath, and without breaking her stride, the girl immediately
said to the principal, "There, Mr. Principal, you missed it. If you had
a video camera, we could have been on America's Funniest Video's!"
-
The classroom should contain visual displays and reminders regarding expected
behaviours and classroom rules, calendars outlining daily jobs and choice
boards. The child with AS will be able to monitor his or her own behaviour
through the use of these visual and concrete clues. Children with AS will:
function with greater success and with less anxiety in an environment
that is orderly, understandable, and predictable both in terms of its macrostructure
(i.e., general arrangement of activities, events, and materials) and in
terms of its microstructure (i.e., inclusion of specific concrete supports).
(Twatchman, 1995, p. 144)
-
Children with AS will need subtle social cues pointed out to them, as they
will not perceive these social cues on their own. There are several types
of social behaviours that may appear confusing for the high-functioning
child with autism and they can be "indexed" (Twatchman, 1995, p.148) or
pointed out for the child. Twatchman gives examples of the different types
of social cues that need to be indexed for the child with autism:
1.point out social information: "Look, Timmy's waving
to you. Can you wave back?"
2.point out emotional information: "Mary got hurt. Look, she's
crying, poor Mary. Can you tell Mary 'I'm sorry'?"
3.point out anticipatory information: "Look, Joey's going to
throw the ball. Put your hands up."
4.structure the commenting function: "Look at the bird eating
birdseed. The bird must be hungry."
5.code feelings and reactions: "Ryan's very angry at Joey for
taking the ball. Tell Joey, 'Give me that ball.'"
6.encourage perspective-taking: "Ryan likes his pickle. Look,
Joey hates his pickle. Look at Joey. Joey's making a face that says 'I
hate this pickle.'" (Twatchman, 1995, p.148)
-
Teach the child with AS functional language, such as the word "No"; "Can
I have a break now?"; and, "I need help." By doing this, the teacher empowers
the child and also prevents temper tantrums that may stem from feelings
of frustration and powerlessness.
Hyperlexia and Language Development
Some authors have suggested that hyperlexia is not the same condition
as autism (e.g. Kupperman & Bligh). They therefore propose a different
set of teaching methods specifically for the hyperlexic student. Kupperman
and Bligh provide some general guidelines to follow when hyperlexia. They
include such things as:
use written language to pattern language, to request items and to label
objects, to outline expectations and rules for behaviour teach specific
phrases and provide opportunities to practice new phrases in various contexts
teach how to answer wh questions
teach how to ask wh questions
teach associations (e.g. same & different); cause and effect; and
sequencing
show how to make choices
teach how to describe
teach how to argue appropriately
practice conversation skills
A beautiful, healthy, three year old girl with autism spends a lot
of time looking at herself in the mirror. She makes faces at herself, and
"sings" to her image in the mirror. Many of these "songs" resemble vowel
sounds, although the girl is non-verbal. The speech and language pathologist
gradually shaped these sing-song sounding vowels into a few words, such
as up and down. However, the young girl would only produce
the words while with the speech and language pathologist in the clinical
setting - she could not generalise to other environments.
Observation of Social Skills
Before a program can be developed that will help a child with autism
improve his or her social skills, the practitioner must first carefully
observe the child (Wolfberg, 1995). These observations are important for
several reasons. In order to know where to begin remediation, the program
developer must know exactly what skills the child already possesses. For
example, a child may have the desire to initiate interactions with peers,
as demonstrated by pushing or hitting the other children in order to get
their attention. With this information, the practitioner can then develop
a social skills program that builds on this primitive initiation skill.
Observations of children are important for other reasons as well. Wolfberg
(1995) explained that observing children at play "fosters a greater understanding
and appreciation of each child's unique play characteristics" (p. 204).
Also, through observation, the practitioner will see how the child solves
problems and confrontations with peers. This information will be useful
when developing a social skills program. Examples of observation forms
can be found in Appendix D.
Activity Routines
In order to help high-functioning children with autism, the adults in
the child's environment must delineate and co-ordinate every step in each
social interaction. The expectations for interactions must be clearly identified
for the child (Quill, 1995). The adults trying to help the child must not
assume that the child has prior knowledge and can generalise from one social
experience to another similar experience.
One strategy for helping children with autism is called an activity routine
(Quill, 1995). An activity routine is a "predictable sequence of interactive
turns...a conversational script of what to do and what to say within the
context of a meaningful situation" (p. 175). The child is provided with
repeated opportunities to practice social interactions. The child learns
what social rules apply in a specific situation and why these rules are
important. Flexibility and generalisation skills are introduced once the
child can participate in a predictable social interaction.
There are several steps to follow when developing an activity
routine that will ensure success for the child. The first step is to choose
a naturally motivating activity in which the child will participate. The
situation should include opportunities for the child to interact with other
children and not merely engage in parallel play. Turn-taking games are
ideal situations for developing an activity routine.
A thirteen year old boy with autism, who said very little to anyone,
went on a field trip to West Edmonton Mall. He went on the very fast ride,
called Drop of Doom. The boy very seriously commented after the
ride, "Oh my God!"
The next step involves defining specific objectives for the
child. The teacher or other adult setting up the activity routine must
have a good idea of what typical children do in the same situation. It
is also important to know what existing skills the autistic child has,
and to build upon these skills. The actions and language interactions expected
from the child must be clearly spelled out. For example, in a turn-taking
situation, it may be outlined as an objective that the child will say "Your
turn" and "My turn" appropriately.
The program developers must also clearly outline the sequence of steps
involved in the activity routine. These same steps should be followed every
time the child practices the routine. Having a script or other written
format is also helpful for many children with autism. The children then
learn exactly what to say and when to say it within the structured activity
routine.
Some children with autism may simply memorise the scripted activity
routine. Once the child has had repeated opportunities to practice a new
skill, then flexibility can be introduced. The activity routines and scripts
can be revised to include new situations and new interactions. Parts of
learned scripts can be inserted into new scripts so that the child has
"opportunities to successfully use learned communication under different
conditions and with various interactive partners" (Quill, 1995, p. 178).
See Appendix E for an example of an activity routine (individual schedule).
Peer Tutoring
A four year old boy with autism had a lot of difficulty sitting still
in the school library with his classmates. He was allowed to move around
and to
find his own space for storytime. Now the boy is comfortable sitting
on the outer boundary of the group of children. He will sit still and look
at
the pictures when shown the book.
Another strategy that helps to develop social skills in children
with autism involves the use of peers. Quill (1995) says that peers can
be trained to interact with children with autism. The first step in the
training process is to explain various communication methods and also to
explain any special methods that their autistic friend may use to communicate.
Next, peers are taught, through role-playing techniques, how to initiate
and maintain social interactions with their friend who has autism. The
adults may also model appropriate behaviours for the peers, showing the
peer what to do and what to say in the situation. Gradually the adult support
and guidance is withdrawn, with the goal of promoting naturally motivating
interactions that occur spontaneously.
Many programs designed to teach children with autism appropriate social
skills, use peer tutors, or same-age peers, in the teaching process. This
is done primarily because the social skills will be learned more quickly
and generalise better when they are taught in a natural setting with children
they would typically interact with in their neighbourhoods, schools, etc.,
as opposed to teaching separate skills in an artificial setting such as
the classroom.
Lord (1995) outlines six basic principles that are commonly found in
peer intervention programs. The six principles of peer intervention include
the following:
-
peer interventions must be conducted in a positive environment in which
interactions with same age-mates are pleasurable,
-
peers are supported in their interactions with the autistic children and
adults, but are not directed how to behave,
-
the temporal and physical structure of the group is deliberately varied,
-
sessions must occur with sufficient frequency so that group rapport develops,
autistic students must comprise less than half of the group,
and,
-
set specific goals for each autistic student in the intervention and evaluate
progress after a specified time.
There are many different social skills programs available,
but most will follow these principles to ensure the success of the intervention
program. The basic elements of an intervention program will attempt to
include interesting activities and materials that will motivate the non-autistic
child to interact with the autistic child. The peer tutors should be given
some general guidelines to follow during the interaction periods. However,
in most instances, they will be left alone during the actual interaction
period, in order
to encourage "spontaneous peer interaction"(Lord, 1995, p. 223). The physical
space will be delineated, in order to keep group members in close proximity
and to encourage interactions between the children. In some intervention
programs, the group will focus on a common object or objective, for example,
playing with playdough, playing a game, or making a snack. Finally, an
intervention program should outline some specific goals for each autistic
child in the group in order to measure progress in specific skills.
Integrated Play Groups
Another strategy used in treatment programs for autistic children is
called integrated play groups. This strategy is based on Vygotsky's work
and his statement "that play is an inherently social and collective process"
(Wolfberg, 1995, p. 194). Vygotsky asserted that "the transmission of culture
through social integration is critical to the formation of mind" (p. 194).
Imagination and play facilitate the sharing of common meanings "and appropriate
social knowledge" (p. 194). Integrated play groups are used to bring expert
and novice players together in a structured setting. The teacher or other
adult in charge guides the interactions between the players. The goal of
integrated play groups is to help children with socially inappropriate
behaviours learn appropriate skills from normally developing children.
First Component
There are several components to the integrated play group model (Wolfberg,
1995). These components provide a structure for the teacher or clinician
to follow when developing a program based on the integrated play group
model. The first step in the model is to monitor the play interactions
between the student and his/her peers. By doing this, the teacher or clinician
can look for a match between the student (the novice player), and the peers
(possible expert players).
Second Component
The second component in the integrated play group model is to "scaffold
interaction" (Wolfberg, 1995, p. 207) between the novice and expert players.
There are three levels of support that the teacher/clinician gives to the
novice player in an integrated play group situation. Level 1 support consists
of providing a lot of verbal and physical cues to the child. The teacher/clinician
may have to guide the student in every interaction and prompt every initiation.
Level 2 support consists of giving the child verbal cues only. The teacher/clinician
also physically moves away from the child when possible. A child is operating
at Level 3 when he or she can play successfully with other children without
the teacher's support. The teacher/clinician should remain close to the
play area, however, in case the child indicates that he/she requires assistance
with an interaction.
Third Component
Another component of the integrated play group model consists of providing
"social-communication guidance" (Wolfberg, 1995, p. 208) for both the novice
and
expert players in the play group.
Strategies are taught to the expert players that will enhance their ability
to engage a novice player in play. For example, the expert player may be
taught to call a novice player's name to get his/her attention, and
to touch the person on the arm or obtain eye contact while calling the
person's name.
Another strategy that both expert and novice players could be taught
would be to say "Can I have a turn?" in appropriate situations.
Fourth Component
The final component of the integrated play group model is to provide actual
play guidance for the players. Wolfberg (1995) gives several examples of
strategies that can be used to guide play interactions. They include:
Orienting Strategies....encourage a novice player to simply observe
the other children in play while maintaining distance from them....Mirroring
Actions....children with autism are very responsive to the mirrored actions
of their own behavior by others. This is a fun way for a peer to attract
the attention of a child who is preoccupied in a repetitive activity....Parallel
Play....fosters children's awareness of one another's activities as they
play with similar materials in the same play space....Joint Focus....encourage
them to actively share materials and to informally take turns in play....Joint
Action....guide the children to formally take turns while actively manipulating
the same objects or participating in the same game. Role Enactment....involves
portraying real life activities through conventional actions....Children
who have not yet reached the stage of advanced pretense can enact roles
within the context of sophisticated play themes organized by more experienced
peers....Role-playing....Children take on pretend roles and use objects
in imaginary ways while enacting complex themes and scripts. (p. 210 -
211)
Social Reading Strategies
Social reading strategies are similar to activity routines, but generally
include more information. They are often used in remediation programs for
the high-functioning student with autism. Social reading is the process
of using "situations from a child's actual experience to visually present
social information and teach social skills" (Gray, 1995, p.220). Social
reading includes three components: social stories, social review, and social
assistance. These three components will be discussed in the following sections.
Social Stories
Social stories are narratives that should make clear certain expectations
and behaviours that many AS children lack. They can be written by teachers,
parents, or other professionals involved with the child. They can be used
at school or in the home. They can be used with children who can read and
those who can not read. Gray (1995), a leader in this area, has stated
that:
Social stories are useful for identifying relevant social cues, introducing
new routines and rules, and/or positively defining desired social skills.
In addition, social stories in the school setting can prepare a child for
unexpected situations such as substitute teachers, fire drills, or school
closings. At home, parents may decide to write a social story to prepare
their child for an upcoming event, such as a visit to a relative or a family
vacation, or to introduce a new daily routine. (p. 222)
Writing a social story should not be undertaken lightly. There are several
steps to consider and lot of careful thought must go into a social story.
The
following is a brief discussion of each step in the writing of a social
story:
Target the skill - This is often quite easy to do. It
will be obvious to the adults involved that the child is having difficulty
with some aspect of social interaction with peers.
A young boy with autism would look through another person's eyeglasses
while still on that person's face, when his glasses were not on his face.
Information Gathering - According to Gray (1995), this is the
most critical step in the writing process. Not only does the writer have
to observe and write down everything that occurs in the targeted situation,
but he/she must take note of things that can not be seen. When gathering
information to include in a social story, the writer must record as many
variables as possible that are part of the targeted situation, such as,
noting that all students are expected to put their work away before lining
up for recess.
The next step in the information gathering process is to find out about
things that the writer is not directly observing. That is, he/she must
find out what happens if something unexpected comes up; if a substitute
teacher is present, if the targeted situation happens every day at the
same time, etc. Gray (1995) suggests that the story writer "Look for aspects
of a situation that may change the situation or alter the basic routine"
(p.223).
The final step in the information gathering process is often the most
difficult. The writer must try to see the situation from the child's point
of view. Gray suggests that the writer discuss the situation with the child
if he or she is able to communicate about it successfully. Also, the parents
of the child involved would be very helpful with this part of the information
gathering process. The purpose of this step is to help the writer better
understand what part of the social interaction or behaviour is causing
the problem for the child.
Share Observations - In this part of the process the writer records
all the information gathered into a social story. The social story may
be presented in written format only, in written format with an audiotape,
or recorded on videotape. The format chosen will depend upon the child's
reading ability. The social story may include illustrations or photographs,
however, this may be too distractible for some children with autism.
Gray (1995) suggests a certain format to follow when writing social
stories. Descriptive sentences usually begin a social story. The purpose
of descriptive sentences are to "explain what occurs and why; they paint
the backdrop" (p. 225) for the child. Directive sentences usually follow
descriptive sentences and generally tell the child to do something. Perspective
sentences are interspersed throughout the social story. Perspective sentences
tell the child why a certain behaviour is expected or how someone feels.
For example, when writing a social story about turn-taking during a game,
the writer should clearly tell the child that taking turns when playing
a game is expected because that is how everyone gets to play and join in
and that the teacher feels happy when everyone gets a turn.
Read and Practice the New Skill - Once the social story is written
and a format decided on, it is ready to share with the child. It should
be read with the child several times a day at the beginning. It can be
shared with class members and other adults in the school. Everyone that
may be involved in the social story or in learning the new skill should
have the opportunity to read it with the child. This is important so that
everyone involved is aware of what the child is trying to learn and what
he/she expects from the others.
A four year old boy with autism really wanted to leave his classroom,
however, the teacher did not allow the boy to leave. The boy took the teacher
to the play centre in the classroom and engaged him in play. After a few
minutes of play, the boy felt that the teacher was distracted and quietly
snuck away towards the door, in another attempt to escape the classroom.
In some cases, a change in the child's behaviour will be noticed
soon after the social story has been introduced. Other times, the progress
will be slower. Often the social story will have to be revised and rewritten
because the child may misinterpret some aspect of it or something crucial
was forgotten in the writing process.
Once the child shows mastery of the new skill, the reading of the social
story can be gradually faded. Sometimes it may be useful to rewrite the
story so that it includes basically the same skill, but takes place in
a different setting. Some children may wish to keep their social stories
in a special place in the classroom to review periodically, on their own
. Appendix F contains an example of a social story.
Social Review
The social review is another part of the social reading strategy. The social
review is more suited for older and high-functioning children with autism,
rather than for younger children and lower-functioning children. The child
must be able to communicate and reflect, somehow, about things he/she sees
and hears. The social review follows the same basic steps as the writing
of a social story:
Target the Skill - Again, this will be fairly easy. For a social
review, however, the teacher does not record the targeted skill with paper
and pen, but with a video recorder. The teacher video-tapes the
AS student in a social situation in which the student is behaving inappropriately.
This is the target situation.
Information Gathering - In this step of the social review, the
teacher and student should be in a room by themselves, with the videotaped
target situations. The teacher begins by explaining to the student that
they will be watching a video of his/her class and that they each will
be writing down things that they see on the tape. The teacher and student
watch the video several times with the volume off, each recording things
on paper, such as the objects they see, the people in the room, and what
the people are doing. The teacher must be careful not to express any statements
regarding the emotions of the people in the video; that is, not to interpret
actions and behaviours as feelings. (The teacher would not say "The teacher
is mad.", but may say "The teacher is frowning and shaking her finger.")
The video is then viewed with the volume on. The teacher and student
again record their observations on paper.
Share Observations - In this step, the teacher reviews his/her
written observations along with the student's written comments. The teacher
points out any similarities between their two observations. The teacher
also uses this opportunity to point out the differences or the things that
the student may have missed in viewing the situation. The teacher writes
down the shared observations along with the new information that the student
missed.
When a young women with autism was a young girl, she loved tape -
any kind of tape. She would keep a stash of various kinds of tape in her
socks. Occasionally she would store elastics and tissue in her socks as
well. Now, as a young woman, she keeps tape and tissue in her pockets.
Practice New Skill - The teacher's job in this step
of the social reading process is to guide the student to a new understanding
of what is expected of him/her in the targeted situation. In some cases,
the student will come to this realisation on his/her own. In other cases,
the teacher will have to tell the student exactly what he/she should be
doing. For example, a student may have a problem with raising his or her
hand during class discussions, preferring to shout out answers and contributions
without giving other students a chance to respond. After viewing this target
situation on video-tape, the student may realise that the other students
in the class raise their hands and wait for the classroom teacher to call
their name before responding. Alternatively, perhaps the student would
not be able to 'read' this social situation, even after repeated viewings
of the video-tape. In that case, the teacher would have to tell the student
directly and quite bluntly, exactly what he or she should be doing.
Once the student understands what is expected of him/her, the teacher
can help him/her to practice the new skill. At this point, a social story
may be written to help point out exactly what the student should be doing
in the targeted situation and what to do if something unexpected happens.
Social Assistance Activities
Social assistance activities are techniques designed to help the child
with autism become more independent in social situations. They include
such things as:
-
Modified Classroom Schedule - Most classrooms have a daily schedule
displayed indicating what subject happens at what time. Gray (1995) suggests
that classroom teachers add the words "Usually we have..." (p. 237) to
the top of the schedule. By doing this, the teacher "introduces the possibility
of variations in the routine as part of the schedule" (p. 237).
-
Modified List of Classroom Rules - Most classrooms display a list
of rules, as well. Often these rules are written by the class and teacher
together. Gray (1995) suggests adding 'why' statements to each posted rule
which explain why the rule is important.
-
A Direction Board - Many classroom teachers list directions to follow
for certain activities and routines. Gray (1995) suggests that teachers
laminate direction boards. They can then write in with erasable pen any
additional activities particular to that day. The student with autism then
has a visual reminder that an expected event will be taking place and when
that event is taking place.
-
Computer Conversations - For some children with autism it is beneficial
to hear a conversation as well as see it. Gray (1995) suggests that for
a really important conversation, (for example, one about the child's behaviour),
that the teacher use the computer with the child. The teacher and child
both sit facing the computer. The teacher types his/her part of the conversation
while talking. He/she also types the child's part of the conversation and
responses. The child is given a printed copy of
the conversation at the end of the discussion.
-
Social Reading Folders - This technique is for the child to use
when doing desk work. The AS student is given a regular file folder, in
which the middle portion of the top sheet has been removed. What remains
is approximately a five-centimetre border made from the top sheet of the
file folder. The child inserts the worksheet into the folder so that the
border surrounds it. Gray (1995) suggests that "On the top border is a
written reminder to the child: 'It's okay if I make mistakes. That's how
children learn.' A statement on the bottom border may direct the child
where to place the completed assignment" (p. 238).
-
Social Reading Bookmarks - This is a visual cue for the AS student,
especially useful to use with specific behaviours. The reminder is written
as a brief statement and is recorded on a bookmark which the child places
in a reader or textbook. An example of a reminder might be "I will raise
my hand before I talk" (Gray, 1995, p. 238).
-
Keep Me Posted Notes - This is a simple strategy that a teacher
can use to remind students about appointments coming up in the day. For
example, the student may have an appointment with the speech and language
pathologist later in the morning. The teacher would write a reminder note
on a sticky note and place it on the student's desk. This reminder may
help the student with the transition from the classroom to the therapy
room.
-
Reminder Signs - This is a good strategy for a teacher to use with
a whole classroom; it does not have to be directed just at the child with
autism. For example, the teacher may notice that the autistic child, along
with several other students, are having trouble remembering to raise hands
to speak. The teacher would create a reminder sign to display during targeted
trouble times, and tell students that when the sign is displayed, they
must try extra hard to remember to raise their hands before speaking out
loud.
-
Social Calendars - The social calendar is a very effective tool
to use with the AS student. The teacher writes a behavioural statement
at the top of a monthly calendar. The statement might be "I will finish
my work" (Gray, 1995, p. 239). At the end of each day, the teacher and/or
student writes a short evaluative comment in the square for that day. The
comment might be as simple as writing 'Yes!', or 'I will try again tomorrow.'
The behavioural statement would be changed each month.
Reverse Mainstreaming
Another effective strategy that has been used with AS students is reverse
mainstreaming. Reverse mainstreaming is a strategy developed by Marian
Wooten and Gary B. Mesibov (1986). They have been using this strategy in
their classroom in North Carolina for the last seven years. This program
is now being used in many special-needs classrooms in other parts of that
state.
Rationale
This program is based on the idea that mainstreaming as a concept, is a
good one, however, there are problems with implementation. This is especially
true of children with autism. Mainstreaming of autistic children generally
takes the form of sending them to join regular classes for part of the
school day. Often this fails with these children because:
changes in their routine and environment would make these disruptions
in their schedule difficult to tolerate. In addition, the activities would
be structured by the teachers in the nonhandicapped classrooms and might
not be appropriate for the skills and abilities of the autistic students.
(Wooten & Mesibov, 1986, p. 307).
A young girl with autism is self- abusive. She hits herself on the
arms and kicks herself on the legs, leaving huge, discoloured bruises.
The young girl will then comment on the colour of these bruises - she pulls
up her sleeves or pant legs, points to the bruise, and says, "Purple."
In order to avoid these problems with regular mainstreaming,
the program developers employ the concept of reverse mainstreaming. Reverse
mainstreaming is simply bringing non-handicapped students into the special-needs
classroom, rather than placing the handicapped students in the regular
classroom. The program developers stress the importance of keeping as many
variables constant as possible for the children with autism. In reverse
mainstreaming, the special-needs students practice skills they already
possess in a familiar environment. The only new variable is the presence
of non-handicapped peers.
Procedure
Wooten and Mesibov (1986) describe one year of this program and the results
of using such a strategy. In the particular year described in their article,
six boys with autism, between the ages of eight and twelve years were involved
with grade five students from the same school. The objectives for each
autistic student differed; each boy had his own individual goals to work
towards. However, the general objective of the program was to improve the
social skills of the children with autism. Examples of specific objectives
included playing Bingo with non-handicapped peers, tolerating the presence
of other children and learning to complete a puzzle in co-operation with
a non-handicapped student.
The regular grade five students came into the special-needs classroom
three times a week. Groups of regular students signed up for a 5 - 6 week
placement in the program. At the end of the 5 - 6 session, a new group
of regular students joined the program. Each regular student was paired
with a special-needs student. The activities that all the children took
part in were cooking, table games, and outdoor games. The non-handicapped
students helped the autistic students with specific goals for each activity.
For example, during a cooking activity, a grade five student's job might
be to teach the autistic child how to stir a bowl of batter. The non-handicapped
student might work on turn-taking or moving only one game piece in a table
game activity. The sports that were included in the outdoor games were
basketball, kickball, croquet, soccer, and baseball. In each sport, the
skills were broken down into
A young boy with autism liked to climb. One day, during a gym class,
he teacher and teacher associate could not find the boy. He had climbed,
unnoticed, to the top of a cupboard unit and was found, curled up, on the
top shelf, happily watching all the action.
component mini-skills. The grade five students were to help the autistic
students learn such things as bouncing a ball, shooting at the basketball
net, etc.
The authors state that there were two rules that all the children
had to follow when working together. Rule one was that everyone was to
call each other by name. The teachers felt that this was important, so
that the special-needs students would have peers to say hello to in the
hallways. Rule two was that the autistic children were to do as much as
they could on their own. In other words, the non-handicapped students were
not to do things for the handicapped students, rather, they were
encouraged to show them how to do something if they required help.
Results
The program developers conclude their description of this strategy by discussing
the benefits of it. They stated that:
as a result of bringing nonhandicapped children into our classroom and
structuring the desired interactions, our students have learned to use
their skills in a meaningful way in naturally occurring situations. This
had led to the acquisition and generalization of these skills and their
use in a variety of settings. In addition, it provided a desirable and
extremely rewarding experience for our children, the nonhandicapped peers,
the families and our school. (Wooten & Mesibov, 1986, p. 318 - 319)
The authors also list some unforeseen benefits of reverse mainstreaming
that occurred for their students. Regular education students began coming
into their special-needs classroom during the day to talk to the students.
Also, the students with autism were asked to eat with "friends" in the
cafeteria at lunch times. Wooten and Mesibov (1986) state that as a result
of this reverse mainstreaming strategy, "greater integration into the community
and school system has become a realistic objective" (p. 318).
Miscellaneous Strategies
There are a variety of programs, ideas and strategies, besides the ones
already mentioned, that can used to improve the social skills and play
skills of children with autism. The following are a few miscellaneous ideas
that may be helpful for some students.
-
Use a coloured circle with the words My Turn printed on it when
children are playing turn-taking games or developing conversational skills.
The circle is passed from child to child to indicate whose turn it is in
the activity.
-
Act out nursery rhymes and fairy tales with props. This will help to increase
the comprehension of stories, improves comprehension of specific words,
and encourages turn-taking.
-
Read predictable story books and pattern stories with children. This will
help to increase general comprehension and increase vocabulary skills.
Examples of such books are: Brown Bear, Brown Bear, The Very
Hungry Caterpillar, and I Know An Old Lady Who Swallowed A Fly.
(See Appendix G for complete references for these books.)
-
Barrier games are excellent activities to do with verbal children with
autism and their non-handicapped peers. They can use two sets of identical
toys (e.g. dolls, furniture, blocks, cars, etc.), or it can be a paper
and pencil activity. Each child has a set of toys and they sit across from
each other with some kind of barrier between them. One child has to direct
the other child to set up the toys in exactly the same positions as his
own, using verbal cues only. This activity develops interactive skills,
employs language repair strategies and increases vocabulary skills.
Behavior Modification Techniques and Current Treatment Programs
A non-verbal, fifteen year old girl with autism, really likes to play
with strings. She spends a lot of time twirling strings in her fingers,
especially shoe laces. One day, the girl's teacher attempted to twirl a
shoe lace in the same manner as the young girl, but the teacher could not.
The girl took the lace away from the teacher and very patiently instructed
the teacher in the art of shoe lace twirling.
There is extensive literature outlining behaviour modification
or behaviour management techniques. This paper will not go into great detail
about this area, but will provide a brief summary of some established behaviour
modification practices. The techniques and practices outlined here are
applicable to many kinds of behaviour problems, not those just restricted
to autism. It will become clear, however, from the discussion, that the
unique characteristics of the child or adult with autism will force the
practitioner of the techniques to be imaginative and at times, unconventional,
in the administration of them! In the following section, I will use the
term "child" or "children" when discussing remediation techniques, however,
many of these same tactics will be effective when used with adults with
autism as well.
Behaviour Management
The following behaviour management techniques are adapted from the work
of Schreibman (1994):
-
Positive Reinforcement - This is when the practitioner rewards a
behaviour by presenting a positive reinforcer immediately after the behaviour.
This technique strengthens the behaviour.
-
Negative Reinforcement - This is when a negative reinforcer follows
immediately after the behaviour. A negative reinforcement usually means
the child is trying to escape or avoid a negative event (e.g. a child might
engage in self-abuse in order to avoid completion of a task because he
or she has learned that when they self-abuse, the demand is dropped - the
self-abuse becomes rewarding for the child). This technique also strengthens
a behaviour.
-
Prompting - Prompting of a skill is used when a child or adult with
autism has no existing skill that needs retraining in the first place.
Prompting is used to encourage and guide the child to develop a new skill.
Schreibman (1994) stresses that "The only requirement of prompts is that
they be functional in leading to the correct performance of the behaviour
(i.e., they must work) and that they ultimately be removed or 'faded' so
that the individual can perform the response unprompted" (p. 17).
-
Shaping - This technique is also used to teach new skills to the
person with autism. In shaping, the practitioner reinforces approximations
to the correct response. Gradually, the child is rewarded for responses
that more closely resemble the correct response, until the desired response
is produced by the child.
-
Chaining - With chaining, the practitioner breaks the target task
into component parts and teaches the child each step one at a time, until
he or she can complete the entire task independently.
Whenever a young eight-year old girl with autism is disciplined,
even in the mildest way, she always strikes out at staff. However, she
strikes out at other staff members, not at the one who scolded her.
-
Extinction - Extinction is a very effective method for decreasing
or eliminating a behaviour. In extinction, the practitioner simply stops
rewarding the inappropriate behaviour. For example, some children with
autism engage in tantrums or begin to self-abuse in order to avoid completing
a task or demand. If the practitioner allows the child to stop the task
when these inappropriate behaviours surface, the child is being rewarded
for engaging in those behaviours. With extinction, the practitioner expects
the child to continue with the task or demand, even though he or she may
be having a tantrum or be self-abusing; in other words, the child is not
rewarded for engaging in inappropriate behaviours. It is common, when extinction
is first used with a child, for the child to engage in more inappropriate
behaviours. He or she is attempting to gain the rewards back again. Also,
the extinction process is usually a slow process; the behaviours are eliminated
gradually.
-
Punishment - The use of punishment in behaviour modification is
usually considered to be a "last resort" measure; that is, only used when
everything else has been tried and nothing else will work. Punishment does
not have to be physical in nature. Often, the term punishment is associated
with cruel or inhuman methods of controlling children. Schreibman (1994)
describes punishment quite differently:
When behavior modifiers speak of punishment, they are merely
describing a situation where the occurrence of an undesirable behavior
is followed by an event the individual finds aversive. This event can be
anything from a frown or gentle "no" to more severe aversives such as a
loud "NO" or a spank, and so forth. In fact anything can be a punisher
if the individual does not like it. If a child hates candy, then candy
could serve as a punisher. (p. 19)
An important point to remember when using punishment techniques with
children is that punishment only serves to stop a behaviour. Punishment
does not it in itself, teach new behaviours. Therefore, practitioners must
teach more appropriate behaviours at the same time as using punishment
to decrease inappropriate behaviours. Schreibman (1994) ends her discussion
of punishment by stating that practitioners must strive towards limiting
the use of aversive punishment, whenever possible. She continues with the
following thought:
One must be concerned with preserving the rights and dignity of the
individual. However, we must also be concerned with maximizing the opportunities
available for the individual to participate as fully as possible in the
community and society. It may be the case that if the only currently effective
treatment for a behavior involves an aversive, and we do not make the treatment
available, we may be denying the individual their right to a full and happy
life in society. (p. 27)
-
Overcorrection - Overcorrection procedures requires the child to
engage in some "effortful behavior (aversive stimulus) contingent upon
the target behavior excess" (Schreibman, 1994, p. 20). For example, if
a child purposefully knocks his or her drink on the floor, the practitioner
expects the child to clean up the mess, as well as
to scrub some additional floor space as the overcorrection measure.
Punishment by withdrawal - Punishment by withdrawal is also known
as the response cost method. Quite simply, punishment by withdrawal is
removing something valued by the child after he or she displays inappropriate
behaviour. For example, it is quite common in school settings to "take
away" a child's recess privilege after he or she has engaged in some type
of disruptive behaviour in the classroom.
-
Time-out - The time-out procedure is also commonly used in schools,
and by parents. With time-out, following an inappropriate behaviour, the
child is removed from the setting and not allowed any positive reinforcements
for a specified time period. This specified time period varies from child
to child, but it is common practice to send a child to a time-out setting
for a minimum of 5 minutes to a maximum of 20 minutes. It is important
to make the setting from which the child has been removed more attractive
than the time-out setting. This is especially important for children with
autism. Frequently they want to be left alone and enjoy the time-out setting.
Thus, the time out setting becomes a reward for the child with autism.
-
Non-aversive strategies - There are many ways in which to deal with
the inappropriate behaviours of individuals with autism. Often many programs
focus only on the punishment of these behaviours and many of the treatment
strategies are considered aversive or punitive measures (LaVigna, 1987).
LaVigna proposes that non-aversive strategies can be used in treatment
plans, as opposed to punishment techniques such as time-out and overcorrection.
LaVigna states that "Empirical evidence and clinical experience strongly
support the position that punishment is only rarely if ever needed, even
to solve the most difficult problems" (p. 423). LaVigna outlines some of
the non-aversive strategies that can and should be used in treatment programs
with autistic people:
1. Differential Reinforcement of Alternative Behavior (Alt-R)
- The reinforcement of behaviors that are incompatible with the undesired
response in intensity, duration, or topography.
2. Differential Reinforcement of Low Rates of Responding (DRL) - The
reinforcement of the undesired response only if at least a specified period
of time has elapsed since the last response, or only if fewer than a specified
number of the undesired responses occurred during a preceding interval
of time.
3. Differential Reinforcement of Other Behaviors (DRO) - Reinforcement
after a specified period of no undesired responding.
4. Stimulus Control - Establishing the discriminative control of an
undesired behavior, either through differential reinforcement or fading.
5. Instructional Control - The differential reinforcement of those responses
which are in compliance with the verbal instruction presented.
One young man with autism will only eat peanut butter sandwiches cut
in a particular way. He will get upset if the sandwiches are not cut properly.
The comment was made to the mother that his caregivers in the future may
not be so precise in cutting the sandwiches. The mother replied, "I don't
care, as long as I can get him to eat something today."
6. Stimulus Satiation - The continued noncontingent presentation
or availability of a reinforcer that reduces the reinforcer's effectiveness.
7. Additive Procedures - The combination of two or more procedures in
order to reduce or eliminate an undesired behavior.
8. Programming - An instructional sequence designed to help the person
reach certain behavioral objectives based on a functional analysis and
involving the systematic manipulation of stimulus conditions, consequences,
instructional stimuli, and other variables that have a functional relationship
with the behavior. (LaVigna, 1987)
Lovaas' (1981) program was described in Chapter 1. His program consists
of using behaviour modification techniques, such as the ones just described.
Lovaas promotes his methods and techniques as desirable and successful
ways to deal with people with autism. He provides guidelines for practitioners
interested in using his methods with children who are autistic. The following
has been taken from the teaching manual that Lovaas developed:
All persons who consistently interact with developmentally disabled persons
have to learn to be teachers....Set small goals in the beginning so that
both you and your child will be rewarded. Find pleasure in small steps
forward.... Be prepared for much hard work. Protect yourself from burn-out
by forming a "teaching team"....Have your child work for what he wants;
make him responsible....Try not to be frightened or feel guilty by the
child's emotional outbursts or withdrawal. You are the boss, you make the
decisions....Begin by making the child's appearance as normal as possible.
(p. 3 -5)
Self-Injurious Behavior
Self-injurious behaviour (SIB) can be defined as any behaviour that
causes physical damage to the person exhibiting this behaviour (Favell
& Greene, 1980). SIB is often considered to be a learned behaviour,
and the person with autism may continue this destructive behaviour because
it produces some kind of change in the environment which he or she feel
is desirable. Favell and Greene (1980) state that there are three consequences
of SIB that may strengthen or maintain the abusive behaviour. The autistic
person with SIB may receive positive rewards when engaged in self-abuse.
For example, it may be a good way to get either positive or negative attention.
The SIB may be an avoidance
behaviour. The person may engage in SIB when he or she does not want to
do a certain task; "self-injury is rewarded and strengthened by allowing
the individuals to escape or avoid what are to them unpleasant situations"
(Flavell & Greene, 1980, p. 3). And finally, SIB may produce sensory
stimulation that the autistic person may find enjoyable.
There are many treatment programs for people who are self-injurious.
Many programs are based on behaviour modification principles and practices.
It is important to precede a treatment program based on behaviour modification
techniques with a thorough medical examination. In some cases, SIB is exacerbated
by an existing medical condition, for example, an ear infection, allergy
or dental problem. Also, some people who self-abuse cause internal damage
that is not visible to the eye, and should therefore have an examination
to rule out and treat any complications from the SIB. Some examples of
this are eye damage from head banging, internal haemorrhaging from pica
behaviour, or malnutrition from rumination (Iwata, Zarcone, Vollmer &
Smith, 1994).
Flavell and Greene (1980) offer the following behaviour modification
suggestions for practitioners who are setting up treatment programs for
individuals with SIB:
-
Alter the situations in which SIB occurs and extend the periods when SIB
does not happen. The practitioner must observe when the SIB most frequently
occurs and when the person with autism does not engage in SIB.
A young thirteen year old girl with autism is abusive towards others
in her environment. She will head butt, unpredictably, backwards into the
stomachs or chests of her caregivers. She will also slap the face of an
adult when given a task to complete.
For example, does the person engage in SIB before meals? Perhaps he
or she is too hungry to wait until mealtime and a small snack would prevent
the SIB from occurring. It is important to reward the autistic person during
times when SIB is not occurring and to extend these times if possible.
For example, if the person does not usually engage in SIB while playing
with a certain toy or object, perhaps he or she could be allowed to have
this toy during "down times" in the day.
-
Provide stimulation in other ways by enriching the environment. Provide
"constant access to toys and activities that the individual prefers, changing
activities as the individual's preference and attention changes, and eliminating
excessive waiting and 'down-time'' (Flavell & Greene, 1980, p. 18).
It is also important to remember to provide lots of positive interactions
between the teacher and student, professional and client, etc. Use a powerful
reward to strengthen appropriate behaviours and try to withhold the same
rewards following a SIB incident. For example, if a person with autism
enjoys the holding and patting he or she receives after a SIB incident,
perhaps he or she could be held and patted after a few minutes of appropriate
behaviours. Flavell and Greene (1980) assert that "only when the individual
receives more rewards for these behaviors than he or she gets for self-injury
will treatment be successful" (p. 24).
-
Remove rewards for SIB. Try to reduce the attention paid to the person
following a SIB incident. Often the self-injury becomes worse when this
method is utilised, or the improvement is very slow. If the rewarding and
non-rewarding of the SIB is inconsistent, the person may continue to engage
in the self-abuse, looking for the opportunities to be rewarded. Also,
the issue of safety must be considered when this method is utilised. Practitioners
cannot ignore severe self-injury. However, practitioners can try to protect
the individual as much as possible (e.g. helmets, padded tables, etc.),
while paying low-key attention to the behaviour.
A young woman with autism will often come to school with food in
her mouth and keep it there for the whole day.
-
A last resort measure may be to punish the self-abuse. Punishment is typically
only considered when other methods have been tried and have failed, the
self-injury interferes with daily activities and "severe self-injury places
the individual in serious danger of blindness, disfigurement or other harm"
(Flavell & Greene, 1980, p. 31). Punishment should be administered
immediately after a SIB incident, with the intention of reducing the behaviour,
not just interrupting it. Punishers will vary from person to person and
each punishment should be followed by a verbal reprimand such as "No! Don't
hit!" (p. 32). Possible punishers have already been discussed in this handbook.
They include such things as time-out, overcorrection, and aversives.
Treatment for self-injury generally proceeds at a slow pace
and must continue for an indefinite time in order to remain effective.
Treatment must occur in all situations; in the home, school, and community.
Treatment can gradually be reduced or altered to fit more naturally into
the person's life. The main purpose of treatment is to always attempt to
replace self-abusive behaviours with appropriate behaviours.
Self-Restraint
Self-restraint is a phenomenon that sometimes occurs along with self-abusive
behaviours. Self-restraint is defined as "self-initiated confinement incompatible
with SIB or preference for such confinement" (Iwata, Zarcone, Vollmer &
Smith, 1994, p. 144). Self-restraint can take various forms; the individual
may self-restrain by placing his or her arms inside an article of clothing,
such as a shirt or jacket or wrap their arms in towels or other large pieces
of cloth. The individual may hold onto objects, seemingly as a way to prevent
SIB. Or the individual may show a preference for mechanical restraints.
Individuals who practice self-restraint tend to engage in serious self-abuse
when not allowed to self-restrain. Thus, the self-restraining behaviour
may interfere with the treatment of the SIB. Also, continuous self-restraint
can lead to problems with "muscular atrophy, arrested motor development,
limited range of motion, and loss of function" (Iwata et al., 1994, p.
144).
The literature in the area of self-restraint shows that there are primarily
two ways to deal with this behaviour. One method uses the self-restraint
as a reward for longer and longer periods of non-SIB. An example of this
method can be seen in the work of Favell, McGimsey and Jones done in 1978
(as cited in Iwata et al., 1994):
Working with individuals who exhibited a preference for mechanical restraints,
the investigators arranged a contingency in which access to restraints
was available following increasingly longer time intervals during which
the subjects exhibited no SIB. Thus, restraints were used as reinforcers
for the absence of SIB, qualifying the procedure as an example of differential
reinforcement of other behavior... (p. 144)
A second method that has been used in order to eliminate self-restraint
uses the behaviour modification technique of shaping and fading. The self-restraint
behaviour is gradually changed from something totally inappropriate to
something more socially acceptable. For example, researchers:
were able to fade restraints almost completely for two individuals who
self-restrained, wore restraints and exhibited SIB. For one individual,
full-arm splints were gradually shortened and then finally replaced with
tennis wristbands. For the second individual, self-restraint (hands in
pants) was first transferred to another restraint (inflatable arm splints)
and then later faded by reducing the air pressure in the splints. In both
cases, intensive treatment was aimed at strengthening alternative behavior
(play with toys and compliance with training tasks) as restraints were
faded. (Iwata et al., 1994, p. 145)
Drug Therapy
The use of drugs in the treatment of autism and self-injurious behaviours
has been common practice for several years. Temple Grandin (1992) an individual
with autism, testifies to the success of drug therapy for her and advocates
the use of medication for other people with autism. She states that antidepressant
drugs such as Tofranil and Prozac can be effective for high functioning
adolescents and adults with autism. The antidepressant drugs seem to alleviate
the symptoms of anxiety that many people with autism feel: the drugs
"have been very effective in autistics who have obsessive-compulsive
symptoms or obsessive thoughts which race through their heads" (Grandin,
1992, p. 112).
Opiate antagonists have been used in the treatment of
self-abusive behaviours (Iwata, et al., 1994). This class of drugs effectively
increases pain sensitivity in the individual taking the medication. This
makes it a good drug to give to SIB patients because it lowers their pain
threshold. Iwata et al. (1994) have reviewed the literature regarding the
efficacy of opiate antagonists and have concluded that "much of the research
to date has not been well controlled and findings have been mixed, suppression
of SIB with the opiate antagonists has been superior to that found with
other drugs" (p. 152).
Back to Table of Contents
Chapter 3
Case Study
The following chapter contains the case study of a young boy who displays
many of the characteristics of Asperger's syndrome and hyperlexia. This
young boy was followed as part of a study on children with high-functioning
autism.
Back to Table of Contents
FAMILY HISTORY
Current Placement
John is a five year-old boy diagnosed with autism. The initial diagnosis
was made when John was three years old. John currently attends an integrated
preschool, four afternoons per week. John's preschool class consists of
ten normally developing children, and five special needs children including
John. In addition, John attends a swimming class and a music class each
once a week. John's classmates in both swimming and music class are normally
developing, same-age peers. John also participates in a speech and language
class for special needs children, two mornings per week.
Prenatal - Birth History
John's mother reports that her pregnancy with John was considered a
high-risk pregnancy. Contractions were monitored, throughout the pregnancy,
beginning at approximately 20 weeks into the gestation period and were
then monitored continually throughout the pregnancy. John's mother was
hospitalised several times for spotting and contractions during the pregnancy.
The baby arrived late; John's mother delivered at approximately 42 weeks.
The mother reports that it was a difficult birth and forceps were used.
The baby was treated for jaundice, both in the hospital and for several
days after discharge from the hospital. Mother and baby stayed in the hospital
for four to five days.
Developmental History and Delay
The mother reports that John was sitting at six months of age and was
walking by 14 months of age. All developmental milestones were reported
as occurring at the appropriate ages. The one exception was speech and
language. John's language development was delayed. He was a very quiet
baby and his early vocalisations consisted of echolalia. John would repeat
sentences and phrases he heard on television. Also, he would repeat sentences
and questions directed at himself spoken by his parents.
John's parents first thought something might be wrong with John because
of his delayed speech and language. John did begin to talk around the age
of two. His first word was "juice" This differs from typical children,
whose first words might be "mama", "dada", "oh-oh", or "bye-bye". John
also differed from typically developing children in that he did not use
pointing or gestures as a means of requesting items. Many of John's early
words were non-communicative and non-functional. For example, John would
memorise slogans from the grocery store. He was able to recognise all the
letters of the alphabet, many numbers and some commercial logos by the
age of two and one-half. By the age of three and one-half JJjjjjjj J ohn
was a proficient reader. John's parents were doubtful about the initial
diagnosis of autism because John was very sociable and affectionate. This
was not what they understood autism to be at that time. John loved attention.
He seemed very bright. The parents felt John simply had a communication
disorder that would eventually improve.
Strengths
After the initial delay in speech and language, John gradually
developed good oral language and grammar skills. As well, John has displayed
extraordinary reading skills from the age of two. John is able to socialise
, in an appropriate manner, with adults. In fact, John prefers the company
of adults rather than with same age peers.
Family
John's parents are a professional couple. John is an only child.
Back to Table of Contents
DIAGNOSTIC INFORMATION
Two Years Old
In October of 1993, when John was two and one-half years old, a psychologist
evaluated John and noted that his language consisted of echolalia and the
parroting of other's speech. John was also beginning to use two-three word
sentences at this point. The psychologist reported that John could recognise
all 26 letters of the alphabet, many numbers and some logos. John could
also read a few sight words, but did not know the meanings of all the words
he could read.
A physician noted in a report when John was two years-eight months old,
that the baby was treated for several ear infections from birth until the
date of the report. John's parents took him to an allergy specialist when
he was two years and eleven months old. The specialist simply noted that
John was a picky eater.
Three Years Old
The first time the diagnosis of autism was mentioned to the family was
when John was evaluated at another centre. The examining physician noted
that John had difficulty answering questions, especially how and why questions.
The physician noticed that John perseverated on activities such as playing
with the toy Magna-Doodle, and having his mother draw letters and shapes
on a chalkboard. The physician also noted that John did not approach other
children appropriately. Rather, he pushed children away upon meeting them
for the first time. John appeared to display no concept of danger and his
attention was constantly fixed on doors that opened and closed.
John was evaluated by another psychologist when he was three years and
five months old. The psychologist noted that on a reading comprehension
subtest, John scored at the grade two level. This indicated that John had
some understanding of what he could read.
Service Agencies
Between the ages of two and four, John has been involved with many service
agencies. John's mother first reacted to these various agencies with some
amount of frustration. She felt that many professionals were not knowledgeable
enough about high-functioning autism. John's mother has since learned to
be vocal regarding the issues involved in raising a child with high-functioning
autism. In fact, John's mother indicates that advocating for John and searching
for appropriate services for John is a full-time job for her at this point.
Back to Table of Contents
CHARACTERISTICS AND BEHAVIOURS RELATED
TO AUTISM
Social Skills and Social Cues
John's weaknesses include a lack of social interaction skills and weak
comprehension skills, both listening comprehension and reading comprehension.
Because of John's weakness in the area of social interaction, he lacks
certain social skills and the awareness of social rules. This makes it
difficult for John to interact meaningfully and appropriately with same-age
peers. For example, it was observed in the preschool setting that John
rarely spoke to other students in the class. John would engage in some
parallel play, but it was never initiated by John. John preferred to play
by himself on the computer or at the listening centre. John did not enjoy
sharing toys with peers and he did not allow others to play with him.
John also demonstrated several times in the preschool setting that he
lacked understanding of certain social cues. He would occasionally become
demonstrative with another student. This would often involve hugging, tickling
or slapping the child on the back in a friendly manner. In most cases,
the other child would tolerate this behaviour for one or two minutes. After
that, he or she would begin to shrug off John's advances and try to back
away from John. John did not seem to realise what these subtle actions
meant; he would continue with the behaviours until told to stop by an adult.
Obsessions
John will engage in stereotypical handflapping when anxious, as well
as mouth his fingers and hands. Occasionally John has slapped his face
when frustrated, but he has always been able to stop himself when told
by an adult to quit.
John, at one time, greeted people by weight and age, rather than by
name. His special interests include calendars, catalogues, and objects
to weigh and measure. Most of John's fixations and obsessions revolve around
numbers. For example, one day while at school, John was examining a vegetable
seed package. He read out every number on the package and kept telling
the teacher the numbers, disrupting the planned activity. Another time,
John engaged one of the teachers in a conversation regarding people and
how much they weigh. He told the teacher that he weighed 50 pounds and
immediately upon being told that another child weighed 25 pounds, exclaimed,
"She's half as much as me!" He then told the teacher that his father weighed
180 pounds and that was three times as much as 60 pounds.
John also is fascinated with buttons that need to be pushed on computers,
elevators, and electric doors, and the like. It was noted several times
in the preschool that John would dominate the computer keyboard and push
many buttons. He also enjoyed pushing the buttons on the tape recorder
at the listening centre. John would often press an elevator button while
walking down the hall with his class. John's mother reports that John will
often stand beside an electric door and repeatedly push the button that
activates the door. In fact, she often has trouble getting John away from
such doors.
Comprehension
John is a nice-looking, handsome child and is very articulate. Nevertheless,
John often lacks the comprehension to go along with his sophisticated oral
language skills. John's mother is concerned that people who do not know
John will assume that he understands things, when in fact, he does not.
For example, in music class the students were requested to choose a particular
colour and to sing a short verse about that colour. All the students wearing
that colour were to stand up as one child sang the verse. On that particular
day, John was wearing the colours white, grey, and blue.
He needed help finding them on himself and then to stand up at the appropriate
time. John sang the required verse by himself when it was his turn, which
happened to be last. However, he sang, "Who is wearing colours?"
rather than "Who is wearing (a specific colour)?"
Another example of John's comprehension difficulty was noted in a speech
and language class. The class was discussing different types of vehicles.
John was asked if he could identify a picture of a Volkswagen. John could
not, so the teacher explained it to John. In response, John said, "You
know a bug is like an old car - it starts at 25" John was referring to
the number of years; in other words, a car starts out at age 25. It seems
that John was trying to connect the slang term "bug" used to describe the
Volkswagen and the concept of "car". He used his fixation with numbers
to relate the two concepts in his mind.
It was also noted by teachers at the preschool that John did not laugh
at funny sections of stories, poems or movies. This indicates that his
understanding of language varies from the normally developing child of
the same age who is often able to recognise humour in stories.
Perseveration
John will often perservate on a certain activity or even repeat a particular
comment over and over again. For example, one day at preschool, John and
several other students were playing with a toy that made various noises
when certain buttons were pushed. After a short time, the other students
left to find other toys with which to play. John, however, played with
that same toy for twenty minutes by himself. In fact, he only pressed one
button repeatedly.
Fine Motor Co-ordination
John often displays problems with fine motor co-ordination skills. For
example, in preschool, John had difficulty forming some of the letters
of his name with play dough. In fact, he needed a model to copy from and
some hand-over-hand assistance. John also had trouble holding the paintbrush
appropriately and easily while painting at the preschool.
Other Special Characteristics
John is a very interesting child with many interesting characteristics
and behaviours. John's special interest in numbers translates into some
extraordinary abilities not often seen in typical children of the same
age. For example, in preschool, a common winter activity was to record
the daily temperature on a large thermometer and chart. John often would
compare the temperatures and could tell the teacher which was the coldest
day recorded and which days had the same temperatures.
John is fascinated with computers and spent a lot of time on the computer
at the preschool. One day in his speech and language class, the teacher
introduced the CD-ROM to the students. John got very excited about this
and quickly learned the new sequence for operating the program. He was
most concerned with the process of pushing the buttons and changing the
screens. He quickly memorised the symbols which indicated which pictures
on the screen had the option of sound and which did not.
Some of the teachers at the preschool noticed the way John interacted
with peers at the computer at the beginning of the school year. Every time
John had a partner playing at the computer with him, he would constantly
help his partner by placing his hand over his partner's hand, thereby guiding
the button pushing. The teachers would verbally tell John, "It's not your
turn, it's ________'s turn." However, John would continue with this hand-over-hand
behaviour. The staff wondered if John thought that he was engaging
in turn-taking behaviour.
John also has some problems with sensory perception. He sometimes cannot
distinguish between hot and cold. John often does not respond to pain.
For example, John's mother reports that one evening she noticed blisters
that were bleeding on the heels of John's feet. John had worn a pair of
new shoes all day and not once complained of his feet hurting or being
uncomfortable.
John is very rigid in his thinking and will sometimes get quite upset
by events that do not make sense to him. John spends his time at home by
following his mother around the house, asking her endless questions and
wanting to help with her daily chores. He also likes to read the TV. and
VCR. instruction manuals on his own.
Strategies and Educational Practices That Have Helped
The objectives for John's intervention program were fairly simple. The
team working with John decided that three main areas needed to be dealt
with in order for John to begin making progress in the social skills area.
John needs to play with other toys besides the computer during his preschool
class, to learn how to take turns, and to learn how to properly begin a
conversation with his peers.
Some of the strategies used to reach these goals are discussed in the
following sections. See Appendix H for the formal lesson plan used in John's
program.
Integrated Play Group
The integrated play group situation, as described in Chapter 2, did not
work very well with John. Initially John was paired with a same-age peer
from his preschool class, and the two children were guided through a play
scenario. The two major problems with this approach were that the typical
four-year old did not always want to play with John at the time when the
play group was scheduled. Also, the attention span of the typical four-year
old is short and often the peer was ready to leave the play situation before
all the goals were accomplished. It was decided to pair John with a slightly
older, typical child, which worked much better. The older child could sustain
longer play contact, would persevere when John ignored them and could guide
John in the play routines.
Individual Play Schedule
The individual play schedule, also described in Chapter 1, began as a complex
schedule intended to guide John through every minute of the preschool afternoon.
It was soon apparent that this schedule was not working for John. He appeared
uncomfortable with it and did not always co-operate. There seemed to be
far too much detail in the schedule for John. Additionally, it was obvious
that John could follow the regular preschool schedule very well on his
own. Upon reflection, it was decided to use the schedule format only during
free time. It was hoped that this would help John to expand his free time
routines. As it turned out, this modified play schedule was exactly what
John needed. It forced him to play with toys and with other children which
he would not normally do on his own.
A more detailed description of the individual play schedule can be found
in Chapter 2. The individual play schedule falls under the heading of Activity
Routines. The actual play schedule used with John can be found in Appendix
E.
Crafts
John's behaviour and attitude towards the daily craft activity in the preschool
changed drastically about half-way through the year. John began the school
year by showing little interest in completing the craft and he had to be
persuaded to take part in the activity. However, about half-way through
the year, the preschool teacher began demonstrating the day's craft during
Circle Time. He would show the students all the materials required to complete
the craft, and then he would demonstrate each step in the completion of
the craft. John was always attentive during these instructions, and often
would go straight to the craft table as soon as Circle Time was done. Other
times he would choose to play at a centre, but would willingly come to
the craft table when called. John would complete the craft, most times,
independently. At times he would have difficulty completing the craft properly,
because his fine motor skills are immature.
Progress Noted Throughout Preschool Year
Social Skills
John made many gains throughout the year. Much of this progress was in
the area of social skills and peer relationships. John's increased proficiency
in these areas were noticed in the preschool classroom. For example, at
the beginning of the November, John was noticed taking turns at the computer
with another student. John had been prompted to take turns at the beginning
of the play session. He was able to carry on with the turn-taking procedure
for several minutes.
In March it was noted that John was taking turns with one other student
at the computer. This turn-taking episode was not prompted; John and partner
initiated it on their own.
Individual Play Schedule
Perhaps the most notable change in John's behaviour revolved around the
use of the individual play schedule. Before the schedule was introduced,
John would typically occupy his free time at preschool by either playing
by himself on the computer or he would listen to audio tapes, again, by
himself. John would neither initiate any social interactions with same-age
peers, nor would he play with the wide variety of toys available in the
preschool.
The introduction of the individual play schedule forced John to break
away from the isolating routine of sitting alone at the computer or the
tape recorder. Although John had been encouraged before this to increase
his interactions with his peers and his environment, this encouragement
was always delivered verbally to John. John did not respond positively
to verbal commands and suggestions. However, viewing the play choices in
a written format motivated John to try some new activities.
The progress was slow at first. For example, shortly after the individual
play schedule was introduced, John could only be coaxed to leave the tape
recorder and engage in some parallel play for approximately five minutes.
After a few sessions gaining experience with the schedule, John's play
behaviour changed significantly. Gradually, John moved from referring to
the schedule frequently to not needing the concrete, visual aide at all.
By the end of the school year, John would willingly respond to suggestions
presented orally by an adult (e.g. "John, please join us at the craft table."
or "John, would you like to play a game with _______?") John also initiated
social interactions after exposure to the play schedule strategy. He was
noticed in March initiating play on his own. Also in March, he spontaneously
joined another child already involved in a play routine. In May, John rejoined
a group of children, on his own, to continue playing after he had been
called away to complete an art activity.
Future Prospects and Concerns
Educational Needs
John is classified as autistic and consequently will need special consideration
from the school system. There are some strategies and approaches that seem
to work for John and the implementation of them should help John with his
school career. One of the strategies that worked well with John in the
preschool involved transitional aides. John often resisted moving from
one activity to another if not properly prepared. Simply telling John that
in two minutes he would have to move on to another activity seemed to help
to prepare him mentally for that activity. Setting a timer and telling
John that when the timer sounded it was time to move into another activity
was another helpful strategy that the preschool teacher used with John.
John might enjoy participating is some activities that centre around
music. John liked to listen to music in the preschool and often moved his
body in time to the beat. In his community music class, he was able to
learn the beat of various songs after given the opportunity to practice.
Perhaps some one-on-one instruction on a rhythm instrument would be beneficial
for John.
John very rarely participated in group singing activities both at the
preschool and during the community music classes. A social story about
singing in a group may encourage John to participate in this activity more
often. However, it seems that John has difficulty doing two things at once,
especially if one of the activities involves language. John's performance
will have to be monitored if a social story is developed for group singing.
John may not learn this skill quickly because it involves language.
John may need to use a tool such as an individual play schedule in Kindergarten.
This tool will help John to expand his play skills and will motivate him
to play with his same-age peers.
Parental Concerns
John's parents want him to be happy when he grows up, regardless of what
career path he chooses. They want him to have friends and to get along
with his peers. Their nightmare for John would be for him to be socially
isolated, to be looked on as strange and to be made fun of by others.
The long-term prognosis made by a psychologist when John was three and
one-half years old indicated that John will likely make good progress in
many areas, because he is only mildly handicapped. The psychologist stated
in the report, however, that John may always be socially awkward and even
possibly socially isolated as he grows up.
Back to Table of Contents
References
Aaron, P.G. (1989). Dyslexia and hyperlexia. The Netherlands:
Kluwer Academic Publishers.
Aarons, M., & Gittens, T. (1992). The handbook of autism a guide
for parents and professionals. London: Tavistock/Routledge.
American Psychiatric Association. (1994). Diagnostic and statistical
manual of mental disorders (4th ed.). Washington,
DC: Author.
Baron-Cohen, S. (1995). Mindblindness: An essay on autism and theory
of mind. Cambridge, Massachusetts: The MIT Press.
Bettelheim, B. (1967). The empty fortress. New York: The Free
Press.
Cole, M., John-Steiner, V., Scribner, S., & Souberman, E. (Eds.).
(1978). L.S. Vygotsky mind in society. Cambridge, Massachusetts:
Harvard University Press.
Delacato, C.H. (1974). The ultimate stranger the autistic child.
California: Academic Therapy Publications.
DeMeyer, M., Barton, S., Alpern, G.D., Kimberlin, C., Allen, J., Yang,
E., & Steele, R. (1974). The measured intelligence of autistic children.
Journal
of autism and childhood schizophrenia, 4, 42 - 60.
Elliott, D.E., & Needleman, R.M. (1976). The syndrome of hyperlexia.
Brain
and Language, 3, 339 - 349.
Favell, J.E., & Greene, J.W. (1980). How to treat self-injurious
behavior. Austin, Texas: Pre-ed.
Frith, U. (1989). Autism explaining the enigma. Oxford: Blackwell.
Frith, U. (Ed.). (1991). Autism and Asperger syndrome. Cambridge:
Cambridge University Press.
Fromkin, V., & Rodman, R. (1993). An introduction to language
fifth edition. Orlando, Florida: Harcourt Brace
Jovanovich, Inc.
Gordon, P., & Lawton, D. (1984). A guide to English educational
terms. New York: Schocken Books.
Grandin, T. (1992). An inside view of autism. In E. Schopler, &
G.B. Mesibov, (Eds.), High-functioning
individuals with autism )pp. 105 - 16). New York: Plenum Press.
Grandin, T. (1995). The learning style of people with autism: An autobiography.
In K. Quill (Ed.), Teaching
children with autism: Strategies to enhance communication and socialization
(pp. 33 - 52). New York:
Delmar Publishers Inc.
Gray, C.A. (1995). Teaching children with autism to "read" social situations.
In K. Quill (Ed.), Teaching children with autism: Strategies to
enhance communication and socialization (pp. 219 - 241). New York: Delmar
Publisher Inc.
Healy, J.M. (1982). The enigma of hyperlexia. Reading Research Quarterly,
3, 319 - 338.
Hinerman, P.S. (1983). Teaching autistic children to communicate.
Maryland: Aspen Systems Corporation.
Iwata, B.A., Zarcone, J.B., Vollmer, T.R., & Smith, R.G. (1994).
Assessment and treatment of self-injurious behavior. In E. Schopler &
G.B. Mesibov (Eds.), Behavioral issues in autism (pp. 131 - 159).
New York: Plenum Press.
Jarrold, C., Boucher, J., & Smith, P. (1993). Symbolic play in autism:
A review. Journal of Autism and developmental disorders, 23,
(2), 281 - 307.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous
Child, 2, 217 - 250.
Kanner, L. (1944). Early infantile autism. Journal of Pediatrics,
6, 211 - 217.
Kauffman, J.M. (1993). Characteristics of emotional and behavioral
disorders of children and youth (5th ed.). New York: Macmillan Publishing
Company.
Kupperman, P., & Bligh, S. The syndrome of hyperlexia: Remediation
techniques[Brochure]. Elmhurst, IL: Center for Speech and Language
Disorders.
LaVigna, G.W. (1987). Nonaversive strategies for managing behavior problems.
In D.J. Cohen & A.M.
Donnellan (Eds.), Handbook of autism and pervasive developmental disorders
(pp. 418 - 429).
Maryland: V.H. Winston & Sons.
Levy, S. (1988). Identifying high-functioning children with autism.
Bloominton IN: Indiana Resource Center for
Autism, Indiana University.
Lord, C. (1995). Facilitating social inclusion examples from peer intervention
programs. In E. Schopler, & G.B. Mesibov, (Eds.), Learning
and cognition in autism, (pp. 221 - 240). New York: Plenum Press.
Lovaas, O.I. (1981). Teaching developmentally disabled children:
The me book. Baltimore, Maryland: University Park Press.
Lovaas, O.I. (1987). Behavioral treatment and normal educational and
intellectual functioning in young autistic children. Journal of Consulting
and Clinical Psychology, 55, 3 - 9.
Lovaas, I., Newson, C., & Hickman, C. (1987). Self stimulatory behavior
and perceptual reinforcement. Journal of Applied Behavior Analysis,
20, 45 - 68.
Lovaas, O.I., Koegal, R.L., & Schreibman, L. (1979). Stimulus overselectivity
in autism: A review of research. Psychological Bulletin, 86, 1236
- 1254.
Lovaas, O.I., Smith, T., & McEachin, J. (1989). Clarifying comments
on the young autism study: Reply to Schopler, Short, and Mesibov. Journal
of Consulting and Clinical Psychology, 57, 165 - 167.
McLennan, J.D., Lord, C., & Schopler, E. (1993). Sex differences
in higher functioning people with autism. Journal of Autism and Developmental
Disorders, 23, (2), 217 - 227).
Moss, G. (1994, September). Hyperlexia. ChicagoParent, 21 - 26.
Olley, J.G. (1992). Autism: Historical overview, definition, and characteristics.
In D. Berkell (Ed.), Autism: Identification, education, and treatment
(pp. 3 - 20). New Jersey: Lawrence Erlbaum Associates, Publishers.
Park, C.C. (1982). The siege: The first eight years of an autistic
child. Boston: Little, Brown and Company.
Powell. T.H., Hecimovic, A., & Christensen, L. (1992). Meeting
the unique needs of families. In D. Berkell (Ed.), Autism: Identification,
education, and treatment (pp. 187 - 224). New Jersey: Lawrence Erlbaum
Associates, Publishers.
Quill, K.A. (Ed.). (1995). Teaching children with autism: Strategies
to enhance communication and socialization. New York: Delmar Publishers
Inc.
Rimland, B. (1964). Infantile autism: The syndrome and its implications
for a neural theory of behavior. New York: Appleton-Century-Crofts.
Sacks, O. (1995). An anthropologist on Mars seven paradoxical tales.
Toronto: Alfred A. Knopf Canada.
Schopler, E., Short, A., & Mesibov, G. (1989). Relation of behavioral
treatment to "normal functioning": Comment on Lovaas. Journal of Consulting
and Clinical Psychology, 57, 162 - 164.
Schreibman, L. (1994). General principles of behavior management. In
E. Schopler & G.B. Mesibov (Eds.), Behavioral issues in autism
(pp. 11 - 38). New York: Plenum Press.
Steli, A. (1991). Sound of a miracle a child's triumph over autism.
New York: Doubleday.
Stone, W.L., & LaGreca, A.M. (1986). The development of social skills
in children. In E. Schopler, & G.B. Mesibov (Eds.), Social Behavior
in Autism (pp. 35 - 60). New York: Plenum Press.
Szatmari, P., Bartolucci, G., & Bremner, R. (1989). Asperger's syndrome
and autism: Comparison of early history and outcome. Developmental Medicine
and Child Neurology, 31, 709 - 720.
Szatmari,P., Bartolucci, G., Bremner, R., Bond, S., & Rich, S. (1989).
A follow-up study of high-functioning autistic children. Journal of
Autism and Developmental Disorders, 19, 213 - 225.
Szatmari, P., Bremner, R., & Nagy, J. (1989). Asperger's syndrome:
A review of clinical features. Canadian Journal of Psychiatry, 34, 554
- 560.
Tsai, L.Y., & Ghazuiddin, M. (1992). Biomedical research in autism.
In D. Berkell (Ed.), Autism: Identification, education, and treatment
(pp. 53 - 74). New Jersey: Lawrence Erlbaum Associates, Publishers.
Twatchtman, D. (1995). Methods to enhance communication in verbal children.
In K. Quills (Ed.), Teaching children with autism: Strategies to enhance
communication and socialization (pp. 133 - 162). New York: Delmar Publishers
Inc.
Van Osdol, B. (1972). Vocabulary in special education. Tulsa,
Oklahoma: The University of Tulsa.
Wallach, G.P. & Miller, L. (1988). Language intervention and
academic success. Austin, Texas: Pro-ed, Inc.
Williams, D. (1992). Nobody, nowhere: The extraordinary autobiography
of an autistic. New York: Times Books.
Williams, K. (1995). Understanding the student with Asperger syndrome:
Guidelines for teachers. Focus on Autistic Behavior, 9 - 16.
Wing, L. (1981). Asperger's syndrome: A clinical account. Psychological
Medicine, 11, 115 - 129.
Wing, L. (1992). Manifestations of social problems in high-functioning
autistic people. In E. Schopler, & G.B. Mesibov (Eds.), High-Functioning
individuals with autism (pp. 129 - 142). New York: Plenum Press.
Wolfberg, P.J. (1995). Enhancing children's play. In K. Quill (Ed.),
Teaching
children with autism: Strategies to enhance communication and socialization
(pp. 193 - 216). New York: Delmar Publishers, Inc.
Wooten, M., 7 Mesibov, G.B. (1986). Social skills training for elementary
school autistic children with normal peers. In E. Schopler and G.B. Mesibov
(Eds.), Social behavior in autism (pp. 305 - 319. New York: Plenum
Press.
Back to Table of Contents
Bibliography
The following books are not listed in the Reference section. They are,
however, useful resources for anyone interested in the field of autism.
Amenta, C.A. (1992). Russell is extra special: A book about autism
for children. New York: Magination Press.
Eastham, M. (1990). Silent words - a biography. Ottawa, Ont.:
Oliver-Pate.
Jordan, R. (1995). Understanding and teaching children with autism.
New York: J. Wiley.
Kaufman, B.N. (1976). Son rise. New York: Harper & Row, Publishers.
Leuchter, S. (1994). Autism and P.D.D.: Using a social stories strategy
for practical problem-solving. Communication Exchange, 5, (3), 8
- 11.
Pinney, R., & Schlachter, M. (1983). Bobby: Breakthrough of a
special child. New York: St. Martin's/Marek.
Sargent, L.R. (1991). Social skills for school and community.
Des Moines, Iowa: The Division on Mental Retardation of the Council for
Exceptional Children.
Schopler, E., & Mesibov, G.B. (Eds.). (1983). Autism in adolescents
and adults. New York: Plenum Press.
Simons, J., & Oishi, S. (1987). The hidden child: The Linwood
method for reaching the autistic child. Rockville, MD: Woodbine House.
Williams, D. (1994). Somebody somewhere: Breaking free from the world
of autism. New York: Times Books.
Back to Table of Contents
Appendix A
Diagnostic Criteria for Autistic Disorder
Diagnostic Criteria for 299.00 Autistic disorder
A. A total of six (or more) items from (1), (2) and (3), with at least
two from (1), and one each from (2) and (3):
(1) qualitative impairment in social interaction, as manifested by at
least two of the following
(a) marked impairment in the use of multiple nonverbal behaviours such
as eye-to-eye gaze, facial expression, body postures, and gestures to regulate
social interaction
(b) failure to develop peer relationships appropriate to developmental
level
(c) a lack of spontaneous seeking to share enjoyment, interests, or
achievements with other people (e.g. by a lack of showing, bringing, or
pointing out objects of interest)
(d) lack of social or emotional reciprocity
(2) qualitative impairments in communication as manifested by
at least one of the following:
(a) delay in, or total lack of, the development of spoken language
(not accompanied by an attempt to compensate through alternative modes
of communication sucy as gesture or mime)
(b) in individuals with adequate speech, marked impairment in the ability
to initiate or sustain a conversation with others
(c) stereotyped and repetitive use of language or idiosyncratic language
(d) lack of varied, spontaneous make-believe play or social imitaative
play appropriate to developmental level
(3) restricted repetitive and stereotyped patterns of behavior, interests,
and activities, as manifested by at least one oft he following:
(a) encompassing preoccupation with one or more stereotyped and restructed
patterns of interest that is abnormal either in intensity or focus
(b) apparently inflexible adherence to specific, nonfunctional routines
or rituals
(c) stereotyped and repetitive motor mannerisms (e.g., hand or finger
flapping or twisting, or complex whole-body movements)
(d) persistent preoccupation with parts of objects
B. Delays or abnormal functioning in at leas one of the followng areas,
with onest prior to age 3 years: (1) social interaction, (2) language as
used in social communication, or (3) symbolic or imaginative play.
C. The disturbance is not better accounted for by Rett's Disorder or
Childhood Disintegrative Disorder.
FROM:
American Psychiatric Association. (1994) Diagnostic and statistical
manual of mental disorders (4th ed.). Washington,
DC: Author. (p. 70 - 71)
Back to Table of Contents
Appendix B
Diagnostic Criteria for Asperger's Disorder
A. Qualitative impairment in social interaction, as manifested by at
least two of the following:
(1) marked inpairment int he use of multiple nonverbal behariors such
as eye-to-eye gaze, facial expression, body postures and gestures to regulate
social interaction
(2) failure to develop peer relationships appropriate to developmental
level
(3) a lack of spontaneous seeking to share enjoyment, interests, or
achievements with other people (e.g. by a lack of showing, bringing, or
pointing out objects of interest to other people)
(4) lack of social or emotional reciprocity.
B. Restricted repetitive and stereotyped patterns of behavior, interests,
and activities, as manifested by at least one of the following:
(1) encompassing preoccupation with one or more stereotyped and restricted
patterns of interest that is abnormal either in intensity or focus
(2) apparently inflexible adherence to specific, nonfunctional routines
or rituals
(3) stereotyped and repetitive motor mannerisms (e.g. hand or finger
flapping or twisting, or complex whole-body movements)
(4) persistent preoccupation with parts of objects.
C. The disturbance causes clinically significant impairment in social,
occupational, or other important areas of functioning.
D. There is no clinically significant general delay in language (e.g.
single words used by age 2 years, communicative phrases used by age 3 years).
E. There is no clinically significant delay in cognitive development
or in the development of age-appropriate self-help skills, adaptive behavior
(other that in social interaction), and curiosity about the environment
in childhood.
F. Criteria are not met for another specific Pervasive Developmental
Disorder or Schizophrenia.
From:
American Psychiatric Association. (1994). Diagnostic and statistical
manual of mental disorders (4th ed.). Washington DC: Author. (p.77)
Back to Table of Contents
Appendix C
Diagnostic Criteria for Mental Retardation
A. Significantly subaverage intellectual functioning: an IQ or approximately
70 or below on an individually administered IQ test (for infants, a clinical
judgment of significantly subaverage intellectual functioning).
B. concurrent deficits or impairments in present adaptive functioning
(i.e., the person's effectiveness in meeting the standards expected for
his or her age by his or her cultural group) in at least two of the following
areas: communication, self-care, home living, social/interpersonal skills,
use of community resources, self-direction, functional academic sklls,
work, leisure, health and safety.
C. The onset is before age 18 years.
Code based on degree of severity reflecting level of intellectual
impairment:
317 Mild Mental Retardation
IQ level 50-55 to approximately 70
318.0 Moderate Mental Retardation
IQ level 35-40 to 50-55
318.1 Severe Mental Retardation
IQ level 20-25 to 35-40
318.2 Profound Mental Retardation
IQ level below 20 or 25
319 Mental Retardation, Severity
Unspecified: when there is strong presumption of Mental Retardation but
the person's intelligence is untestable by standard tests
from:
American Psychiatric Association. (1994). Diagnostic and statistical
manual of mental disorders (4th ed.). Washington DC: Author. (p.77)
Back to Table of Contents
Appendix D
Individual Preschool Schedule
The individual preschool schedule was initially designed to encompass the
complete preschool program. After some experimenting with the schedule,
it became obvious that John did not need a schedule to guide him for the
whole afternoon of preschool; he was able to follow the teacher's instructions
and he did participate in most activities. However, he did seem to need
extra guidance during the Free Time portion of the preschool program. John
would typically choose activities that required little or no interaction
with peers. For example, John would usually choose to play on the computer
or go to the listening centre during Free Time. He would not respond to
suggestions to play with other toys or to join other students in different
activities.
The individual schedule, or script, as outlined below, is the initial
draft that encompasses the whole preschool program. After a few sessions,
the majority of the statements were removed from the schedule. Only statements
pertaining to the use of Free Time were kept in the schedule.
Each of the following statements were printed on separate 8.5 x 5.5
pieces of paper. Each preschool day, nine of the statements were selected
and inserted into plastic pockets mounted on yellow bristol board. Initially,
the preschool teacher or teacher associate decided which statements would
be included in John's schedule. Eventually, John was given more control
over the procedure and was allowed to choose which activities he would
participate in for each school day. Each section of the preschool was coloured
coded. All the statements and choices for Free Time have one particular
coloured sticker attached to them, all the statements for gym class have
a different coloured sticker on them, etc.
Some statements were deliberately created with blank spaces in them
in order to allow for flexibility for the preschool staff. The teacher
has the option of filling in the blanks to suit the activities that are
planned for a particular day.
The statements that appeared on John's individual schedule are:
I will say hello to one student.
I will say hello to Tom (the teacher) and the teacher associate.
I will go to the other preschool classroom and sing songs.
I will go to ________ to ________.
I will play with the vehicles.
I will play on the computer.
I will help make soup.
I will help bake muffins.
I will help bake cookies.
I will help make ________.
I will ask a friend to play ________ with me.
I will play with puzzles.
I will play at the water table.
I will look at books.
I will build with the blocks.
I will paint at the paint easel.
I will play in the house corner today.
I will play in the sandbox.
I will listen to a tape at the listening centre.
I will dress up in the play clothes.
I will swing on the tire swing outside.
I will slide down the hill on a toboggan.
I will play on the slide and bridge outside.
I will cut paper using the scissors at the table.
I will paint at the table.
I will do the ________ craft.
I will sit on the toilet before I wash my hands.
I will wash my hands using soap.
I will wash my hands for snack without getting my sleeves wet.
I will set out the glasses for snack because I am the special helper.
I will set at the table for snack after I wash my hands.
I will choose a book or puzzle after I put my glass in the sink.
In the gym I will ask a friend to ________ with me.
In the gym I will play on the teeter-totter.
I will play the game in the gym.
In the gym I will climb the ladder and go down the slide.
In the gym I will play with a ball.
In the gym I will crawl through the tunnel.
I will try the actions for the songs at Circle Time.
I will try singing the songs at Circle Time.
I will choose one book in the library today.
I will listen to Tom read a story in the library.
I will follow the directions in my locker when it is time to go outside.
Individual Schedule for Home
The following statements appeared on a home schedule devised by John's
mother and the early intervention worker:
I will get up and go to Mom and Dad's room to say hello.
I will go to my room to take off my clothes.
My clothes are laid out on my bed and I put on my clothes.
I pick up my dirty clothes and put them in the laundry basket.
Mom calls me to the table for breakfast.
I eat breakfast.
I tell Mom that I am finished and Mom and I go into the bathroom to
get washed up.
I have free time until Mom says it is time to go.
I go to the living room and sit on the couch and read a book or watch
TV.
Mom says it is time to go to language class/music class/swimming class.
I go to the front door and read my GET READY cards.
Individual Arriving and Departing Schedule
for Preschool
The following statements were printed on cards which were attached to
wall of John's locker at the preschool. They were visual reminders for
appropriate arriving and departing behaviours. The statements were:
| Arrival at Preschool |
Departure from Preschool |
| I take off my gloves |
I take off my shoes. |
|
Hat |
I put on my
boots |
|
coat |
coat |
|
boots |
hat |
| I put on my shoes. |
gloves. |
| I go into the classroom. |
I sit and wait. |
Back to Table of Contents
Appendix E
Social Story for Taking Turns at the Computer
(Page 1) My name is John. I go to preschool at the 123 School.
Tom is my preschool teacher. Sometimes Tom lets us play on the computer
during Free time.
(Page 2) Sometimes I choose to play on the computer. Somtimes
I play by myself. Sometimes other children join me at the computer.
Other children come to the computer because they want to play too.
When someone else comes to the computer, we well take turns pressing buttons
or using the mouse.
(Page 3) When another child is pushing a button or using the mouse,
I keep my hands on my lap and wait for my turn. Sometimes I know
the answer, but I will let the other person answer the question.
When the other person is done, then it will be my turn.
(Page 4) Sometimes there may be three or four of us at the computer.
Two children will be on the chairs, playing the computer game. The
other children are just watching us play. My friend and I will take
turns playing the game. I keep my hands on my lap while I wait for
my turn.
(Page 5) We take turns on the computer because everyone at the computer
will have fun when each person gets a turn. Taking turns is one thing
friends do for each other. Tom is happy when we take turns on the
computer.
Note: This social story was printed on yellow paper, in
large letters, laminated and inserted into a binder. This social
story was shared with his whole preschool class.
Back to Table of Contents
Appendix F
Special Bibliography
The following books were mentioned in Chapter 2, under the heading of
Miscellaneous
Strategies. These predictable storybooks can be used to help
increase a child's vocabulary and comprehension skills. the books
mentioned in Chapter 2 are:
1. Brown Bear, Brown Bear, What Do You See?
Bill Martin
H. Holt & Co., New York
1983
2. The Very Hungry Caterpillar
Eric Carle
The World Publishing Co., New York
1969
3. I Know an Old Lady Who Swallowed a Fly
Abner Graboff
Rand McNally, Illinois.
1961
Back to Table of Contents
Appendix G
Lesson Plan
October 23, 1995
OBJECTIVES:
1.John will expand his toy repertoire to include toys available
in the preschool, other than playing with only at the computer.
2.John will learn some strategies for turn-taking on the computer and
also in other situations that require turn-taking skills.
3.John will learn some strategies for initiating a conversation with
peers.
PROCEDURES:
1.The teacher associate will encourage John to play with toys
other than the computer. The teacher associate will invite other students
to join with John in playing with toys available in the preschool such
as blocks, cars and Duplo. The teacher associate will guide the play situations
using the suggestions outlined in the section on integrated play groups
found in the 1995 book, Teaching Children with Autism: Strategies to
Enhance Communication and Socialization, by Kathleen Quill. (p. 206
- 214)
2.The teacher associate will help John learn turn-taking skills through
the use of social stories.
3.The teacher associate will help John learn conversation initiation
skills through the use of social stories.
4.The teacher associate will help John with organisational skills through
the use of an individual schedule.
Back to Table of Contents